
If you want to skip the backstory and just get to the instructions, click here.
If you’re a paid subscriber and you want to learn about more effective options than Ozempic or about sources with verified quality, click here.
Wegovy (Ozempic, Semaglutide)1 was found to be extremely effective for safely achieving weight loss and subsequently approved for its treatment in 2021. Since then, it’s enjoyed a level of popularity like no other drug before it. In fact, the whole class of drugs—GLP-1 receptor agonists, or just GLP-1s—has enjoyed skyrocketing popularity. In early 2024, the Kaiser Family Foundation polled Americans about their GLP-1 drug usage and reported that one-in-eight had used the drugs at least once.

With that popularity came shortages: manufacturers simply could not keep up with Americans’ demand for safe and effective weight loss medication. When the FDA declared that there were GLP-1 shortages, that meant that millions of Americans made their first contact with compounding pharmacies, because a shortage meant these pharmacies were cleared to produce and sell their own preparations of these drugs.

When compounding pharmacies started selling their own Ozempic, they definitely alleviated the shortages, and they worked to make the drugs far more available than they would be otherwise, in two main ways:
Several of these pharmacies provided a process for would-be users to obtain prescriptions for GLP-1 drugs. It’s an open secret that this process was more lenient than the typical prescription process that takes place at a doctor’s office.
Compounding pharmacies offered much lower costs for many potential GLP-1 users because insurance coverage of GLP-1 drugs is spotty. These users would have had to choose between paying upwards of $1,000 per month or $300 via compounding pharmacies. At the former price, the drugs were often unaffordable.
But now, the FDA has declared that the shortages are over, so the compounding pharmacies no longer have the right to sell compounded GLP-1 drugs. Ironically, the end of the shortage therefore means greatly reduced GLP-1 access for millions of Americans who came to depend on compounding pharmacies for their access.
But access doesn’t have to be cut off. Plenty of people have discovered that GLP-1 drugs are easy to prepare yourself. While I legally cannot and I do not recommend doing that, those who want to can follow the steps below to accomplish that goal.
How To Get Very Cheap Ozempic
Step one in getting very cheap Ozempic is to find a peptide source. There are tons of these online and you can find them by Googling things like “buy Ozempic peptide”. Lots of reliable sources come up on the first page with that search, but if you want to see my preferred source, go to the section after this one. A bottle of Ozempic peptide looks like this:

Using my preferred source, you get 31 weeks of Ozempic using the typical dosing schedule for $501.5 total, or $64.71 per month. After getting to week 17, the per-month price rises to $96.3 per month (assuming a month = four weeks) because you’re using 2.4 mg per week—about one-third what compounding pharmacies were selling for. Do note: It is possible to do better than this price (i.e., $19 per month), but the purity guarantees doing that are inferior, so I cannot say I ‘prefer’ or ‘recommend’ that in any sense. Adventurous people can still choose to do that if they so wish! [Update: My ‘preferred’ source linked below sells Ozempic for $15.47/month.]

Once you’ve found a source and ordered your peptides, let’s talk storage. Before reconstitution, I recommend keeping them in the freezer. This extends their shelf life from months to years. After reconstitution, do not freeze them, but do refrigerate them when you’re not actively trying to use them. If your refrigerator is so cold that it freezes a reconstituted peptide, you’re making a mistake. Now to be clear, you do not need to keep them refrigerated when you’re drawing from your vials either, refrigeration is just for when you’re not preparing an injection.
With peptides in hand, you’ll still need to order a few more things before you can inject yourself. Luckily, those things are cheap, legal, and readily available. You’ll need:
Bacteriostatic water. This is crucial for preparing your Ozempic and you can get it on Amazon, or often enough, from peptide sources themselves. Bacteriostatic water can be kept at room temperature until opened, whereafter it should be refrigerated.
Sterile syringes. These are going to be used for transporting bacteriostatic water and Ozempic. They are very cheaply available in bulk on Amazon, Aliexpress, and through many other online retailers. I recommend getting 1 mL syringes for pulling from your vials and injecting and 3 mL syringes for putting bacteriostatic water in.
Sterile needles. These are going to be used for penetrating your bottle of Ozempic, your bottle of bacteriostatic water, and your fat butt2 (or stomach, or arms, or wherever you feel most comfortable injecting). They’re readily available on Amazon, Aliexpress, and elsewhere, like the other ingredients are. I recommend 4mm needles at 30 or 32 gauge for adding bacteriostatic water to your Ozempic and for pulling Ozempic from your vials, and 34 gauge needles (higher gauge = thinner needle) for injecting, but the size of needles you use is up to your personal preference.
Sterile swabs. Any old alcohol swabs will tend to do. You can get these at Walmart and other superstores, on Amazon, Aliexpress, and in so many other places. If you’re the sort of person to own a first aid kit (which you should be), then you probably already have a lot of these in your home. If not, just buy them; they’re extremely cheap.
And that’s all you’ll need. If you’re a judicious shopper, it should cost you about $40 to get all of this in sufficient quantities to go for a year or more. If you’re not good at finding good prices, I could see someone paying $60 for this or more if they’re buying very large quantities of this stuff for whatever reason. Do your shopping right and this should add no more than $3 per month to your Ozempic bill.
Now that you’ve acquired your peptides and all the tools you need, it’s time to reconstitute your peptide. This simply means turning them from a crystallized form to a liquid one that you can inject. You start by getting out one of your vials of your Ozempic peptide and another vial of your bacteriostatic water. They will have caps on them, like the red cap in the illustration below. Take those off. Do not take off the metal cap with the gray plastic on top of it. That’s the sterile barrier.

Now prepare a syringe. Grab one of your syringes and pull back the quantity of air equal to the amount of bacteriostatic water you want to pull from your bottle. This amount will vary depending on how much of the peptide is in your vials, but for the formulation I recommend, I supply quantities in the section below. This information will always be trivial to calculate, but if you’re having trouble, Google it. Put a needle for drawing out bacteriostatic water on it, and grab an alcohol swab. You’re going to use the alcohol swab on your bacteriostatic water vial’s lid before you put the needle through the bottle’s gray plastic part on the lid. Next, push in the air and draw back the required amount of water.
Now that you have your bacteriostatic water drawn into your syringe, take the needle out and use a fresh alcohol swab on the vial for your peptide. Put in the needle with the bacteriostatic water and inject the water before removing the needle and disposing of it and the syringe safely, meaning not letting a needle just lie loose. If you have stable hands, put the cap back on the needle before disposal; if you do not, then don’t bother with recapping it, because you might prick yourself, and that can suck. To dispose of a needle safely, place it in hard-sided container with a lid, such as a food storage box or an empty laundry detergent canister.
Wait a moment until there are no more chunks in your bottle, at most gently swishing around your peptide. Once you just see a clear liquid, you have reconstituted Ozempic! Now it’s time to get it in your body.
Take a fresh syringe and needle and pull back the quantity of air equal to the quantity of Ozempic you want to draw, swab down the top of the vial (do this each time you need to prick it), put your needle on your syringe, and pierce through the top of the vial and draw the quantity of Ozempic you want. Once you’re done, pull out the needle and dispose of it safely, before putting on a fresh needle. Now onto injection.
When you have a prepared needle and syringe, you just need to alcohol swab your injection site thoroughly and put the needle in and inject. It’s that simple, but if you’re not familiar with how to do this, just look it up online. There are tons of video guides to do this. The injection site can be any appropriate subcutaneous fat injection site, but I recommend injecting into belly fat, because for most people, that’s the easiest way to do this. If you’re lean enough that it’s not the easiest site for you, then search around for an appropriate site.
And that’s all it takes! Go store the remaining part of your vial, and you’re done. If you did everything right, you just prepared and injected cheap, high-quality, homemade Ozempic. Congratulations on the biohacking.
Ozempic Is Not The Top GLP-1 Drug
If better priced sources than the ones linked below emerge, I will provide links to those as soon as I’m aware of them.
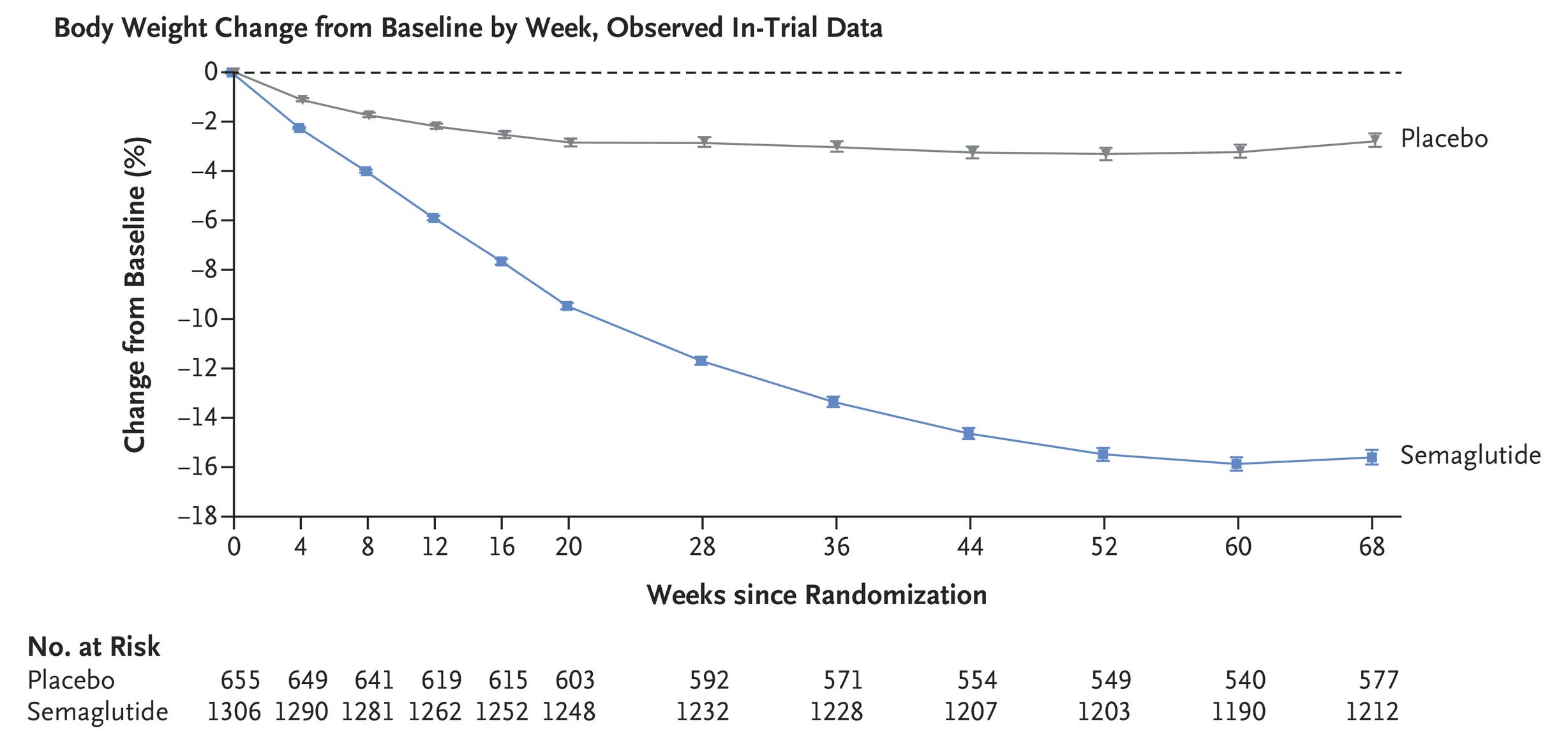
Ozempic produces staggering weight loss. Compared to a lifestyle intervention and a placebo injection, a lifestyle intervention plus Ozempic3 led to a 15% reduction in bodyweight in this trial. Other trials show similar results.
But Tirzepatide (Mounjaro, Zepbound) produces even more weight loss, and greater health benefits too.
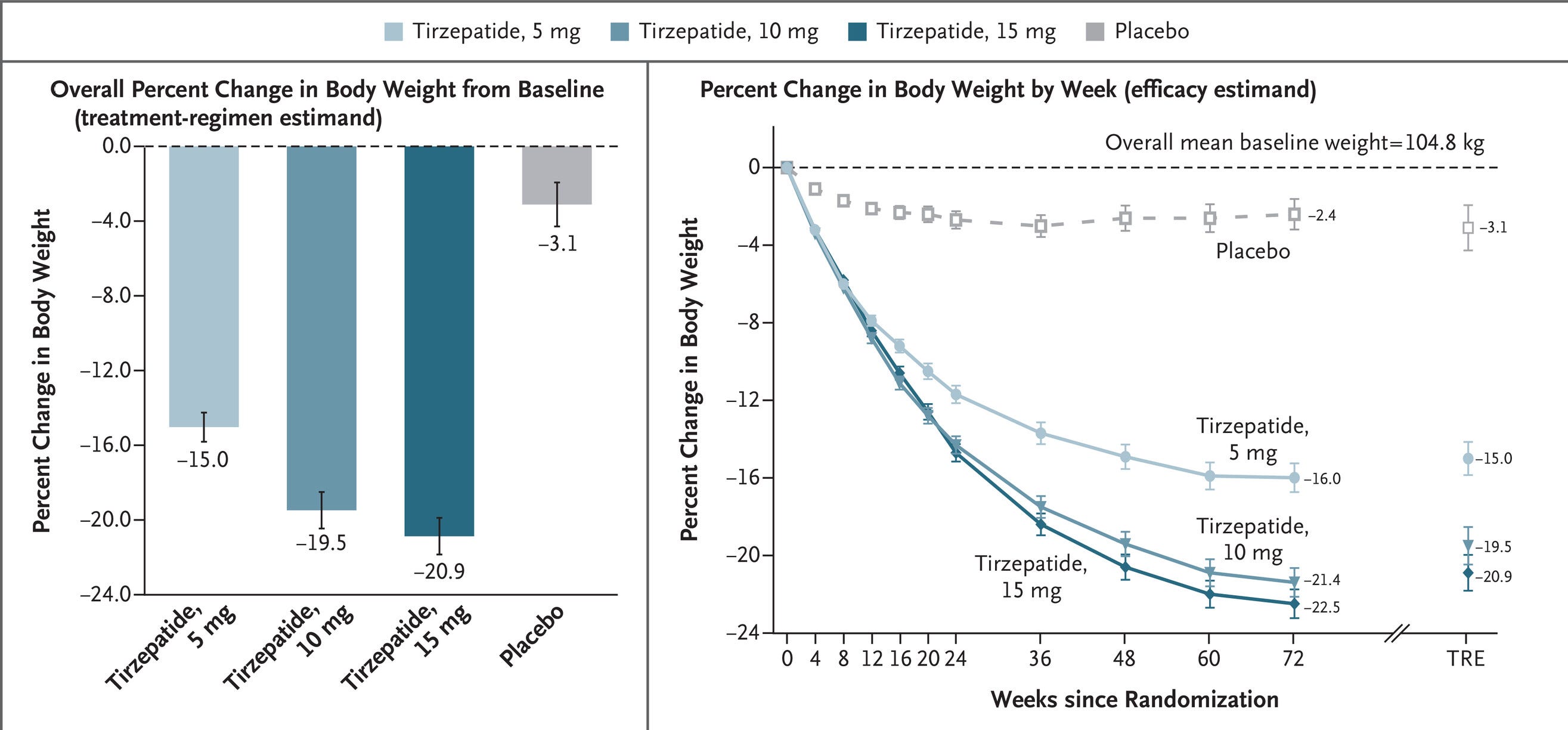
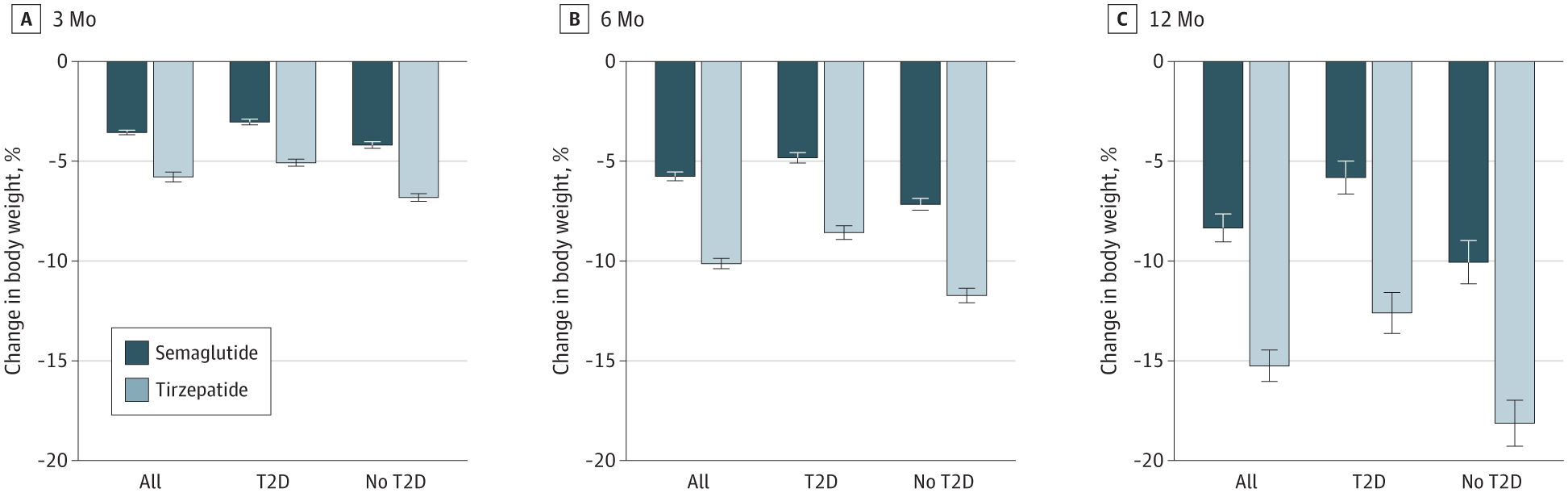
Compared head-to-head using propensity score matching, Tirzepatide consistently beats Ozempic, as you would expect when contrasting trial results.
Tirzepatide is, for all intents and purposes, Ozempic Plus. It has a similar primary GLP-1 receptor agonist-based method of action, but it also adds another ingredient: GIP, or gastric inhibitory polypeptide, a weak inhibitor of gastric acid secretion and another insulin secretion stimulator. This makes Tirzepatide more effective, but adding an ingredient does increase the a priori odds of side effects. Anecdotally, I have known two women who had mental side effects on Tirzepatide that they did not have when they used Ozempic. On the other hand, people have told me that their memory improved with GIP, which was actually a predicted side effect based on how it works.
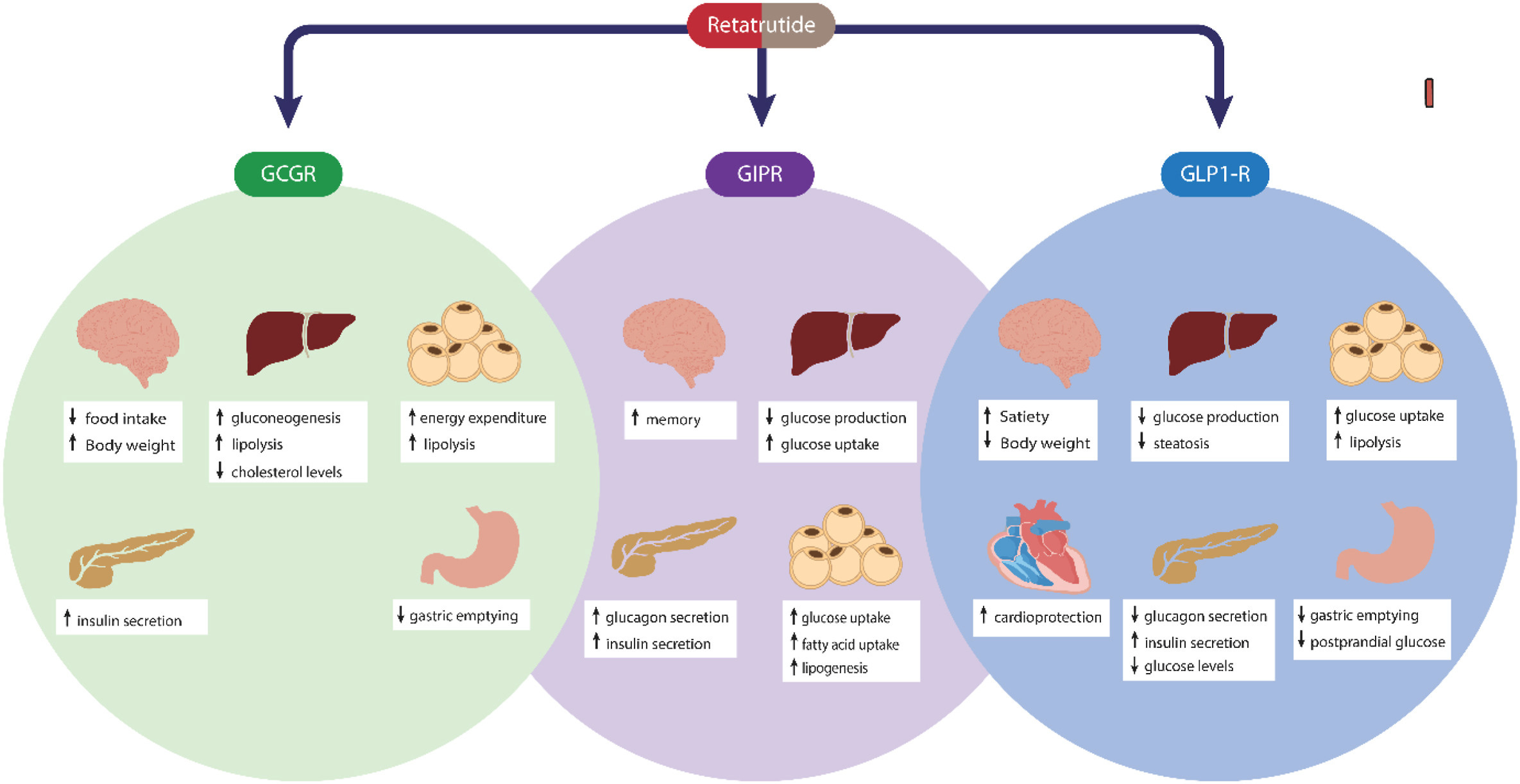
But Tirzepatide is not the top GLP-1 drug. That title currently goes to Retatrutide, which is basically Tirzepatide Plus. Like Tirzepatide, Retatrutide contains a GLP-1 receptor agonist, GIP, and it also adds in glucagon, resulting in some interesting effects that are particularly pronounced in the liver. In fact, one phase 2 trial found that Retatrutide has excellent effects on markers of liver health.
Other trials confirm extensive weight loss benefits. The weight loss impact even seems to be larger than those for Tirzepatide or Ozempic.

And why shouldn’t it be? Retatrutide is lean mass sparing, meaning that what loss happens has even more to do with fat than occurs with Ozempic or Tirzepatide. Retatrutide is also metabolism boosting and metabolism sparing. Where weight loss tends to lead to decreased metabolism, becoming harder and harder as it continues, Retatrutide blunts that effect. In one particularly revealing experiment, mice were injected with Retatrutide or nothing and subjected to the same diets and temperatures. The Retatrutide mice lost 35% of their body weight while the matched mice lost just 20%. When Retatrutide-treated mice were treated with glucagon antibody antagonists, this added weight loss effect stopped. Exploration reveals that Retatrutide increases fat mass reduction through increased lipid oxidation, supplementing energy levels, leading to maintained locomotor activity. Perhaps this is also related to why it seems to reduce visceral (belly) fat so selectively.
The wonders of this drug go on and on. It really is incredible, and anecdotally, people report to me that it’s more tolerable than both Tirzepatide and Ozempic. I don’t know if that will hold up, but I will note that the trial results suggest limited side effects. [Edit: Retatrutide does show a cardiac safety signal. This may be due to the added glucagon, but that’s not clear quite yet. This is not worth worrying too much about unless you have a prior history of cardiac issues.]
To obtain Retatrutide, I would (if I were offering this advice) recommend buying from Solution Peptides. They are the source I am currently saying I would recommend because they:
Have verified high quality products. Their product purity is very high.Have the lowest prices I’ve found. With the addition of discount code “heather15” at checkout, orders are marked another 15% off from their already competitive pricing. Usage of that code is how I achieved the $501.5 figure for Ozempic I mentioned earlier.
A 10-vial pack of Retatrutide can be obtained from this link. A 10-vial pack of Ozempic (Semaglutide) can be purchased from this link. This source also sells bacteriostatic water with pricing that is very competitive, even before applying the 15% discount code.
Nexaph. They are a source with an active community, frequent testing, and extremely good prices. Their Easter rate for Retatrutide is 240 mg for $350, which for most Americans, nets out to about $367.50 after shipping and handling. Normally, their rate for the same quantity is $550, which is still an incredible deal that stacks up well compared to other sources that have quality testing going on. Without the 15% off deal from my previous recommended source, Solution Peptides, the $350 deal is 84.5% better, and at $550 for the same amount, it’s 75.8% better.
Nexaph’s price for Semaglutide is even more outrageously low. They’re selling a 100mg kit consisting of 10 10mg vials for $170. At a 2.4mg weekly dose, that nets out to $4.08 dollars per week for almost 42 weeks. I no longer recommend Nexaph. They set up an online community, the community demanded overfilling vials beyond their labeled quantities, and reports have come out showing that they supply much more Retatrutide, Tirzepatide, and Semaglutide than their labeled dosages. For example, in a recent batch of Retatrutide, they labeled the bottles as containing 24mg, but they contained 30-34mg. The product was completely pure, but providing too much means that the bottles cannot be trusted without everyone engaging in testing.
While this is unlikely to cause any meaningful level of harm beyond an upset stomach because of the excellent safety profile of these drugs, it’s still not trustworthy behavior, so I no longer recommend them. If you want more product than you think you’re buying and you’re OK with guesswork or sending off a test bottle or two, then Nexaph will still be fine for you. Now I really don’t recommend Nexaph. Their most recent batch ‘addressed’ the overfill issue by being slightly underfilled by about 10%, and it had subpar, 97.3% purity. I cannot in good conscience recommend them until they return to at least 99% purity. I realize purity issues are not entirely their fault, but I can see that this has a lot to do with rushing to meet demand. They will need to earn back trust.
Peptide Partners. This source is credible and is selling Retatrutide, Tirzepatide, and Semaglutide at reasonable prices. For Retatrutide, someone using a 4mg weekly dose would end up paying $41.60 per month at their prices, and if they were to use their Tirzepatide, they would end up paying $130.00 per month with a 15mg weekly dose. Their Semaglutide, on the other hand, only costs $18.20 per month at a 2.4mg weekly dose. [Edit: Peptide Partners reached out to give me a discount code for you all to use to get an additional 15% off of your order. The code is ScrewTariffs, and it’s applied in your cart. This drops the monthly prices for Retatrutide, Tirzepatide, and Semaglutide, respectively, to $35.36, $110.50, and $15.47 per month. Edit II: Peptide Partners also uses the 15% discount code doge. I want to reiterate that I like this source for their quality guarantees. For example, they use a domestic lab—TrustPointe in Michigan.]
May 31 update: My new and current recommendation is to vet sources using Finnrick. Finnrick compiles results for various sources and grades them based on purity of the product, the quantity relative to the labeled amount, and the presence of batch identifiers. If companies over- or underfill their vials, they’re penalized; if their product is less pure than desired, they’re penalized; if there are no batch identifiers, they’re penalized. This is a good way to do things. This does not grade on price, so I will continue providing price-based recommendations as well, but if those are not up to date, you can search for price information by clicking through sites reviewed by Finnrick.
June 17 update: If you want a strong quality guarantee with a somewhat higher price, I recommend looking through the top of Finnrick’s list. Solution Peptides is also still good, and their prices remain reasonable, albeit not pack-leading.
I have no financial interest in these sources (original post source: Solution Peptides; second post source: Nexaph; third post source: Peptide Partners; fourth post source: Pure Rawz; fifth post source: Finnrick’s list), am not using any sort of referral link, do not benefit from any discount codes, and am not profiting from this in the slightest. I am not even recommending this be done in the first place. If another source comes up that is priced better, with as much data to indicate its product quality, I will recommend that source instead. And remember, sources can always go from offering good product to bad product in the blink of an eye; I am not assuming responsibility for product quality changes.
If you purchase a 10mg vial of Retatrutide from any source, like Solution Peptides, the mixing instructions are simple. Just add 2mL of bacteriostatic water for reconstitution, and then if you want to inject a typical dose that I’ve seen people use with high efficacy, inject 0.4mL for 2mg a week. If you elect to use their cheap Ozempic instead, the amount of bacteriostatic water to add is also 2mL.
This post should have made clear just how easy it is to avoid the Ozempocalypse.
June 18 2025 Update: Titration Schedules
Titration is optional, but important to maximize the benefits of GLP-1RAs while keeping their side effects in check. People who fail to step up their dosages cautiously risk side effects that range from annoying to serious. Of course, stepping up dosages at all is optional; no one is being compelled to increase their dosage from a bare minimum quantity. Ultimately, the choice to do so is up to the user, and where they end up dosage-wise is a matter of personal discretion. People generally see larger effects at higher doses, with considerably diminishing effects outside of current dosage schedules.
In order to minimize side effects, semaglutide is prescribed with the following dosage schedule, reprinted from above:
Tirzepatide, on the other hand, is quite a different chemical, and its equivalent dosage schedule looks like this:

Retatrutide lacks an FDA approval at the moment. As a result, there is no published recommended dosage schedule. Following in the style of the tirzepatide chart, this is what I’ve gathered to be the likely dosage schedule for retatrutide when it’s finally released. This chart is based on testimony from trial participants and long-time users. It does not reflect a recommendation so much as what I believe to be the likely dosage schedule.
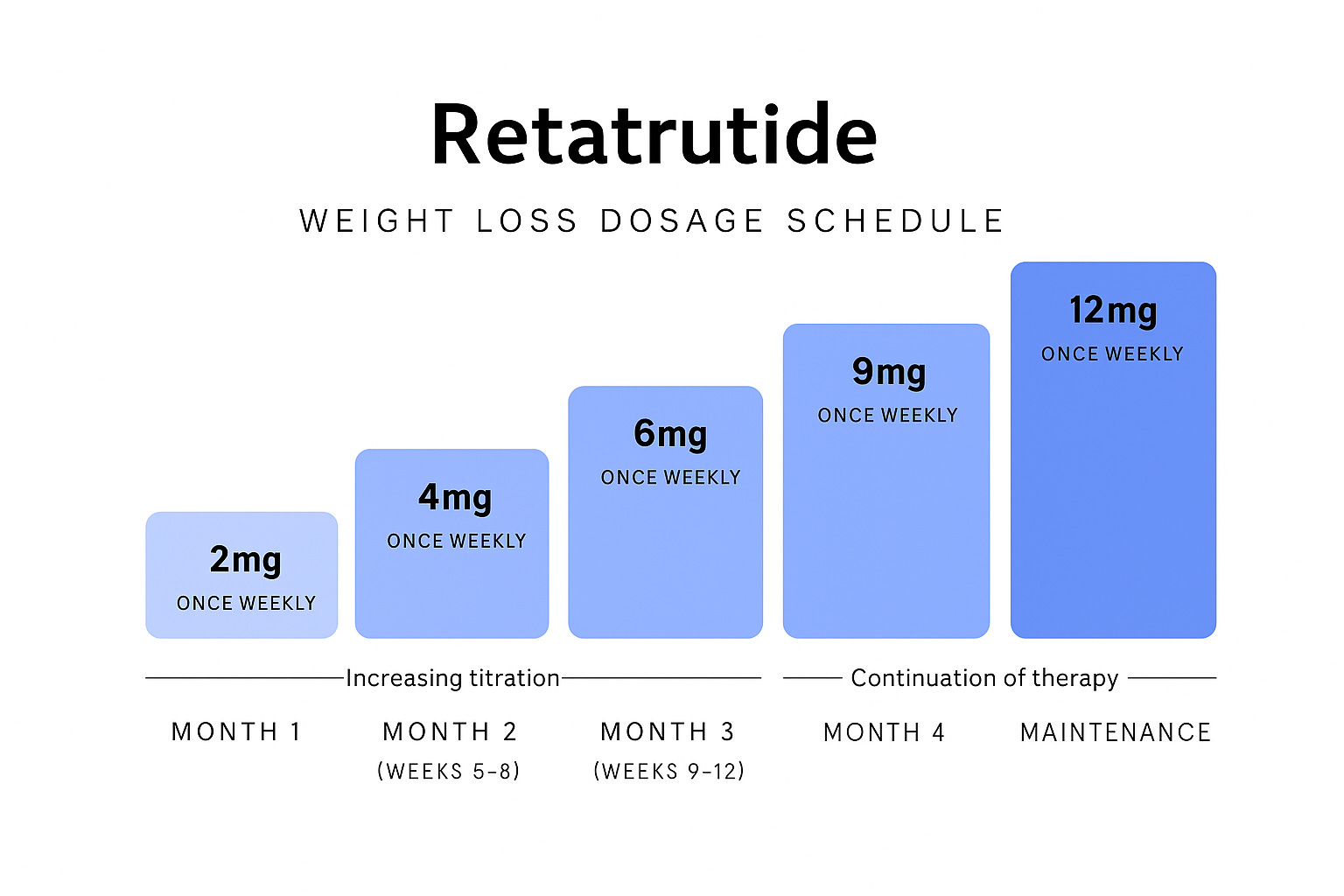
This dosage schedule is speculative, and when an official one is released, I will post an update here. Individuals who are lighter, or often enough just female, may prefer starting with 1mg. From surveying users, I’ve found that often makes sense and 2mg is too heavy a start for some. Do what works for you, surveil trials to see how people react to different dosages if you feel you need to, and most importantly, do what feels right. At the end of the day, if a certain dosage is too much for you, then dialing it back might be your best move. I hope this dosage schedule chart can be informative.
August 24 2025 Update: Slow Titration and Side Effects
Most of the popularly-hyped side effects of GLP-1RAs are not real (e.g., muscle-wasting, pancreatitis, colorectal and thyroid cancer, major adverse cardiovascular events); are incredibly rare and tied to preexisting conditions (e.g., proliferative retinopathy)4 ; or are exaggerated to high heaven (e.g., gastrointestinal side effects). The most common side effects of GLP-1RAs fit in the last category and they include things like nausea, vomiting, diarrhea, constipation, and delayed gastric emptying (otherwise known as gastroparesis). But, these side effects are:
Almost always non-severe, they might annoy, but they rarely cause serious harm;
Usually fleeting, they come and go fast;
Considerably population-specific;
Rarer on tirzepatide and retatrutide than with semaglutide;
Typically avoidable through slow titration.
These factors are incredibly important, and I’ve made sure to mention them from time-to-time for an important reason: I hate the idea of people irrationally fearing medications that could greatly improve their lives. It just won’t do for people to be afraid of something that could, at once, extend their lifespan, improve their healthspan, and bolster the quality of their life in a variety of ways having to do with aesthetics. So, below, you’ll find a brief review, and then I’ll get into concrete strategies to avoid side effects.
Firstly, if you go and read the primary literature on trials, you will find numerous comments such as: “The most common adverse events in both treatment groups were gastrointestinal, and most were mild to moderate in severity and occurred primarily during dose escalation.” If you read about real-world usage and you see that large numbers of people discontinue using the drugs, again, don’t worry; the reasons for discontinuation are typically socioeconomic, and most people actually get back on the drugs. Clearly the side effects are not commonly bad enough to be considered severe.
Secondly, as many trials have shown, side effects fade out. The quotation above suggests this tends to no longer be an issue after dose escalation (i.e., titration), and that is true. With gastroparesis, both in trials and in preclinical studies, the same is true: it tends to go away fairly quickly. Consider the result of this head-to-head trial comparing semaglutide and tirzepatide:

Moreover, these gastrointestinal side effects are reactive, meaning that they occur based on the things you do while on the drugs. I’ll return to this below.
Third, diabetics and nondiabetics get different effects on these drugs. The effects are usually the same, directionally, but side effects are often quite different. It’s been observed both in the real world and in trials (compare, e.g., SURMOUNT and SURPASS) that diabetics lose less weight on the drugs. It should also be our expectation that diabetics will lose a greater portion of weight as lean muscle mass given their greater insulin resistance. For diabetics, we see that GLP-1RAs are associated with reduced rates of gallstones and ileus constipation, whereas for people who are merely obese, GLP-1RAs are associated with slightly increased rates of both conditions. (But again, these things are only rarely and contingently severe.)
A more important thing to note about diabetic and nondiabetic use of these drugs is that rare, extreme side effects are practically only seen among diabetics. The most common examples of this in the press are microvascular harms—that is, damage to small vessels, and particularly in the eyes. If you check Footnote 3 and what it’s a comment on, you’ll see an example of this. Basically, diabetics can fare poorly with GLP-1RAs for the same reason that they fare poorly with intensive insulin therapies: getting their HbA1c (blood sugar) under control too quickly shocks the body and can cause issues. For diabetics who are already under control, or people who are nondiabetic, this should not be an issue, so there’s no need to fret over it.
Fourth, newer drugs tend to come with fewer side effects and greater efficacy. Older GLP-1RAs like exenatide and liraglutide cause more distress to patients, require greater numbers of injections (unless you’re on a long-acting version), and tend to work worse for glycemic control and weight loss. This is even true comparing semaglutide (as a reminder, that’s the active ingredient in Ozempic/Wegovy) to tirzepatide (the active ingredient in Mounjaro/Zepbound). Consider the rates of vomiting and nausea in comparable trials for both drugs:

Tirzepatide gives a walloping to semaglutide. It is both a more effective drug and a drug with superior safety: fewer and less severe side effects! This is driven by its five-times weaker GLP-1R agonism that seems to happen due to co-occurring GIPR signaling in the hindbrain. This superior side effect profile is why, I’ve found, I can transition friends who struggle with gastrointestinal issues on semaglutide over to tirzepatide or retatrutide (which is broadly similar to tirzepatide in terms of its side effect profile) and see them succeed at substantially higher rates.
Here’s the part you might care more about: How can you lower rates of side effects?
Beyond choosing to use tirzepatide or retatrutide over semaglutide, the first thing to note here is that most side effects of a gastrointestinal nature are reactive. The longest term variety of interaction here is through failing to eat a healthful diet, causing constipation. Normally, with excessive food consumption, you might get enough fiber, for example, but after you cut back on eating, you might get far less, proportionally and totally, leading to blockage. The most important interaction for acute nausea, vomiting, and so on, is with binge eating and drinking. I’ve helped people to overcome issues with these drugs on several dozen occasions now, where the problem was nothing more than that they had a problem of eating beyond the point where they were full. If you eat or drink too much, you’ll feel sick on or off these drugs, it’s just that, off them, the threshold is a lot higher. Keep that in mind.
The second thing to note is that you can prevent most side effects with slow titration. Consider this result from a recent trial of semaglutide. Study the chart:

With a slower increase in dose compared to the typical titration schedule that I’ve shown above, people ended up with less than half the number of days feeling nauseous. That’s huge! This also replicates. For example, here’s a result for tirzepatide:
Further evaluation of [gastrointestinal adverse events, i.e., gastrointestinal side effects] incidence from the first onset data showed that the [adverse events] most probably to occurred following the first dose (4 or 2.5 mg), and the incidence and prevalence may have been reduced with lower starting doses… Also, smaller subsequent dose escalations were more probably associated with a lower incidence of the combined nausea, vomiting and/or diarrhoea [adverse events].
This replicated in other tirzepatide trials, like SURPASS-2:
The dose-escalation scheme in the current trial of the phase 3 SURPASS clinical program, which included a lower starting dose and slower dose escalation in smaller increments, was associated with a better gastrointestinal-related side-effect profile than the scheme in the phase 2 trial, which involved more rapid escalation. Gastrointestinal adverse events reported with tirzepatide and semaglutide were consistent with those that would be expected with the GLP-1 receptor agonist class and were mostly mild to moderate and occurred during the escalation period with both trial drugs.
This slower titration schedule led to fewer discontinuations, fewer total adverse events, and everything else you’d expect if people were hurting less. In the real world, the improved rates and severity of side effects with tirzepatide are associated with better adherence. This result holds up with other GLP-1RAs and with numerous other drugs as well.
So, struggling with side effects? Or worried about struggling with side effects? It’s simple: start small and go slow. Begin your dosing with a low dose and increase gradually. You may not lose weight as quickly with this approach, but you’ll eventually get there without the issue of side effects haunting your way up the dosing ladder. If the trial results are to be believed—and they should be—then you also won’t lose weight that much more slowly with slower titration, so don’t feel like you’re missing out by doing this.
One dosing schedule I’ve been trying out on subscribers involves having them start with 0.5 mg per week of retatrutide and then moving it up by just 0.25 mg per week, until they feel comfortable moving it up more rapidly. This seems to work incredibly, and has helped plenty of people who struggled with normal dosing schedules to actually stick with the drugs without a problem.5
What I encourage you to do, if your aim is avoiding side effects, returning to the drugs without side effects, reducing the extremity of side effects, or any combination or permutation thereof, is to go slow, and if something feels bad, pull back your dose, let it work, and up it again—only if you need to—at a later point. If you do this right, you can trivially use these drugs without meaningful side effects.
I will be referring to Semaglutide and Wegovy by the brand name “Ozempic” throughout this piece because it is popular.
This originally read “fat ass”, but a subscriber asked for profanity to be removed. I’ve now obliged.
Both the placebo and Ozempic groups used the typical dosing schedule for Ozempic, which I showed above.
The proliferative retinopathy exampled I linked used a potentially noncausal design, but its conclusions are supported by trials like SUSTAIN-6.
Another thing I’ve been trying has generated some more marginal improvements for people, and that is to get them to inject smaller amounts twice a week instead of one larger dose once a week. This helps to smooth over circulating levels throughout the week, which might help, but I’m not as confident in this conclusion quite yet, so I’ll leave this as a footnote until I’ve gathered more data.




