As always, some people need practical advice, and we can’t agree on how any of this works and we are all different and our motivations are different, so figuring out the best things to do is difficult. Here are various hopefully useful notes.
John Burn-Murdoch: While we can’t be certain that the new generation of drugs are behind this reversal, it is highly likely. For one, the decline in obesity is steepest among college graduates, the group using them at the highest rate.
This and our other observations are not easy to reconcile with this study, which I note for completeness and shows only 5% average weight loss in obese patients after one year. Which would be a spectacular result for any other drug. There’s a lot of data that says that in real world conditions you do a hell of a lot better on average than 5% here.
Jonel Aleccia: “I have been on Wegovy for a year and a half and have only lost 13 pounds,” said Griffin, who watches her diet, drinks plenty of water and exercises regularly. “I’ve done everything right with no success. It’s discouraging.”
Whether or not that is 13 more pounds than he would have lost otherwise, it’s not the worst outcome, as opposed to the 5 in 5 people who won’t lose weight without GLP-1 drugs. 4 out of 5 is pretty damn exciting. I love those odds.
Eliezer Yudkowsky offers caveats on GLP-1 drugs regarding muscle mass. Even if these concerns turn out to be fully correct, the drugs still seems obviously worthwhile to me for those who need it and where it solves their problems.
He also reports it did not work for him, causing the usual replies full of 101-level suggestions he’s already tried.
I presume it would not work for me, either. Its mechanism does not solve my problems. I actually can control my diet and exercise choices, within certain limits, if only through force of will.
My issue is a stupidly slow metabolism. Enjoying and craving food less wouldn’t help.
That’s the real best argument I know against GLP-1s, that it only works on the motivation and willpower layer, so if you’ve got that layer handled and your problems lie elsewhere, it won’t help you.
Samo Burja: Compelling argument. Papers by lying academics or tweets by grifters pale in comparison.
This is the state of the art in nutrition science and is yet to be surpassed.
I'm embarking on this diet experiment, starting today. 💪
People ask me if I'm on Ozempic, and I say no.
Don't you understand the joy of willpower?
How much should we care about whether we are using willpower?
There are three reasons we could care about this.
Use of willpower cultivates willpower or is otherwise ‘good for you.’
Use of willpower signals willpower.
The positional advantage of willpower is shrinking and we might not like that.
Wayne Burkett: People do this thing where they pretend not to understand why anybody would care that drugs like Ozempic eliminate the need to apply willpower to lose weight, but I think basically everybody understands on some level that the application of willpower is good for the souls of the people who are capable of it.
This is concern one.
There are two conflicting models you see on this.
The more you use willpower, the more you build up your willpower.
The more you use willpower, the more you run out of willpower.
This is where it gets complicated.
There’s almost certainly a short-term cost to using willpower. On days you have to use willpower on eating less, you are going to have less of it, and less overall capacity, for other things. So that’s a point in favor of GLP-1s.
That short-term cost doesn’t ever fully go away. If you’re on a permanent diet, yes it likely eventually gets easier via habits, but it’s a cost you pay every day. I pay it every day, and this definitely uses a substantial portion of my total willpower, despite having pulled this off for over 20 years.
The long-term effect of using willpower and cultivating related habits seems to have a positive effect on some combination of overall willpower and transfer into adjacent domains, and one’s self-image, and so on. You learn a bunch of good meta habits.
If you don’t have to spend the willpower on food, you could instead build up those same meta habits elsewhere, such as on exercise or screen time.
However, eating is often much better at providing motivation for learning to use willpower than alternative options. People might be strictly better off in theory, and still be worse off in practice.
My guess is that for most people, especially most people who have already tried hard to control their weight, this is a net positive effect.
I agree that there are some, especially in younger generations who don’t have the past experience of trying to diet via willpower, and who might decide they don’t need willpower, who might end up a lot worse off.
It’s a risk. But in general we should have a very high bar before we act as if introducing obstacles to people’s lives is net positive for them, or in this case that dieting is net worthwhile ‘willpower homework.’ Especially given that quite a lot of people seem to respond to willpower being necessary to not fail at this, by failing.
Then we get to a mix of the second and third objections.
Wayne Burkett: If you take away that need, then you level everybody else up, but you also level down the people who are well adapted to that need.
That’s probably a net win — not even probably, almost certainly — but it’s silly to pretend not to understand that there’s an element to all these things that’s positional.
An element? Sure. If you look and feel better than those around you, and are healthier than they are, then you have a positional advantage, and are more likely to win competitions than if everyone was equal, and you signal your willpower and all that.
I would argue it is on net rather small portion of the advantages.
My claim is that most of being a healthy weight is an absolute good, not a positional good. The health benefits are yours. The physically feeling better and actually looking better and being able to do more things and have more energy benefits are absolute.
Also, it’s kind of awesome when those around you are all physically healthy and generally more attractive? There are tons of benefits, to you, from that. Yes, relative status will suffer, and that is a real downside for you in competitions, especially winner-take-all competitions (e.g. the Hollywood problem) and when this is otherwise a major factor in hiring.
But you suffer a lot less in dating and other matching markets, and again I think the non-positional goods mostly dominate. If I could turn up or down the health and attractiveness of everyone around me, but I stayed the same, purely for my selfish purposes, I would very much help everyone else out.
I actually say this as someone who does have a substantial amount of my self-image wrapped up in having succeeded in being thin through the use of extreme amounts of willpower, although of course I have other fallbacks available.
A lot of people saying this sort of stuff pretty obviously just don’t have a lot of their personality wrapped up in being thin or in shape and would see this a lot more clearly if a drug were invented that equalized everyone’s IQ. Suddenly they’d be a little nervous about giving everybody equal access to the thing they think makes them special.
“But it’s really bad that these things are positional and we should definitely want to level everybody up” says the guy who is currently positioned at the bottom.
This is a theoretical, but IQ is mostly absolute. And there is a reason it is good advice to never be the smartest person in the room. It would be obviously great to raise everyone up if it didn’t also involve knocking people down.
Would it cost some amount of relative status? Perhaps, but beyond worth it.
In the end, I’m deeply unsympathetic to the second and third concerns above - your willpower advantage will still serve you well, you are not worse off overall, and so on.
In terms of cultivating willpower over the long term, I do have long term concerns we could be importantly limiting opportunities for this, in particular because it provides excellent forms of physical feedback. But mostly I think This Is Fine. We have lots of other opportunities to cultivate willpower. What convinces me is that we’ve already reached a point where it seems most people don’t use food to cultivate willpower. At some point, you are Socrates complaining about the younger generation reading, and you have to get over it.
I buy that the world needs to back up the truck and pay Novo Nordisk the big bucks. They’ve earned it and the incentives are super important to ensure we continue doing research going forward, and we need to honor our commitments. But this does not address several key issues.
The first key issue is that America is paying disproportionately, while others don’t pay their fair share. Together we should pay, and yes America benefits enough that the ‘rational’ thing to do is pick up the check even if others won’t, including others who could afford to.
But that’s also a way to ensure no one else ever pays their share, and that kind of ‘rational’ thinking is not ultimately rational, which is something both strong rationalists and Donald Trump have figured out in different ways. At some point it is a sucker’s game, and we should pay partly on condition that others also pay. Are we at that point with prescription drugs, or GLP-1 inhibitors in particular?
One can also ask whether Tyler’s argument proves too much - is it arguing we should choose to pay double the going market prices? Actively prevent discounting? If we don’t, does that make us ‘the supervillains’? Is this similar to Peter Singer’s argument about the drowning child?
The second key issue is that the incentives this creates are good on the research side, but bad on the consumption side. Monopoly pricing creates large deadweight losses.
The marginal cost of production is low, but the marginal cost of consumption is high, meaning a rather epic deadweight loss triangle from consumers who would benefit from GLP-1s if bought at production cost, but who cannot afford to pay $400 or $1,000 a month. Nor can even the government afford it, at this scale. Since 40% of Americans are obese and these drugs also help with other conditions, it might make sense to put 40% of Americans on GLP-1 drugs, instead of the roughly 10% currently on them.
The solution remains obvious. We should buy out the patents to such drugs.
This solves the consumption side. It removes the deadweight loss triangle from lost consumption. It removes the hardship of those who struggle to pay, as we can then allow generic competition to do its thing and charge near marginal cost. It would be super popular. It uses government’s low financing costs to provide locked-in up front cold hard cash to Novo Nordisk, presumably the best way to get them and others to invest the maximum in more R&D.
There are lots of obvious gains here, for on the order of $100 billion. Cut the check.
If you don’t want to do GLP-1s and you can’t date a sufficiently attractive person, here’s a claim that Keto Has Clearly Failed for Obesity, suggesting that people try keto, low-fat and protein restriction in sequence in case one works for you. Alas, the math here is off, because the experimenter is assuming non-overlapping ‘works for me’ groups (if anything I suspect positive correlation!), so no even if the other %s are right that won’t get you to 80%. The good news is if things get tough you can go for the GLP-1s now.
Bizarre freak that I am on many levels, I’m now building muscle via massive intake of protein shakes, regular lifting workouts to failure and half an hour of daily cardio, and otherwise down to something like 9-10 meals in a week. It is definitely working, but I’m not about to recommend everyone follow in my footsteps. This is life when you are the Greek God of both slow metabolism and sheer willpower.
Aella asks the hard questions. Such as:
Aella: I've mostly given up on trying to force myself to eat vegetables and idk my life still seems to be going fine. Are veggies a psyop? I've never liked them.
Jim Babcock: Veggies look great in observational data because they're the lowest-priority thing in a sort of Maslow's Hierarchy of Foods. People instinctively prioritize: first get enough protein, then enough calories, then enough electrolytes, then... if you don't really need anything, veg.
Eric Schmidt: Psyop.
Psyop. You do need fiber one way or another. And there are a few other ways they seem helpful, and you do need a way to fill up without consuming too many calories. But no, they do not seem in any way necessary, you can absolutely go mostly without them. You’ll effectively pick up small amounts of them anyway without trying.
The key missing element in public health discussions of food, and also discussions of everything else, of course joy and actual human preferences and values.
Stian Westlake: I read a lot of strategies and reports on obesity and health, and it’s striking how few of them mention words like conviviality or deliciousness, or the idea that food is a source of joy, comfort and love.
Tom Chivers: this is such a common theme in public health. You need a term in your equation for the fact that people enjoy things – drinking, eating sweets, whatever – or they look like pure costs with no benefit whatsoever, so the seemingly correct thing to do will always be to reduce them.
Anders Sandberg: The Swedish public health authority recommended reducing screen usage among young people in a report that carefully looked at possible harms, but only cursorily at what the good sides were.
In case you were wondering if that’s a strawman, here’s Stian’s top response:
Mark: Seeing food as a “source of joy, comfort and love?” That mindset sounds like what would be used to rationalize unhealthy choices with respect to quantity and types of food. It sounds like a mantra for obesity.
Food is absolutely one of life’s top sources of joy, comfort and love. People downplay it, and some don’t appreciate it, but it’s definitely top 10, and I’d say it’s top 5. And maybe not overall but on some days, especially when you’re otherwise down or you put in the effort, it can absolutely 100% be top 1.
If I had to choose between ‘food is permanently joyless and actively sad, although not torture or anything, but you’re fit and healthy’ and ‘food is a source of joy, comfort and love, but you don’t feel so good about yourself physically and it’s not your imagination’ then I’d want to choose the first one… but I don’t think the answer is as obvious as some people think, and I’m fortunate I didn’t have to fully make that choice.
One potential fun way to get motivated is to date someone more attractive. Women who are dating more attractive partners had more motivation for losing weight, in the latest ‘you’ll never believe what science found’ study. Which then gets described, because it is 2024, as ‘there might be social factors playing a role in women’s disordered eating’ and an ‘ugly truth’ rather than ‘people respond to incentives.’
Nutrients
Carmen claims that to get most of the nutrients from produce what matters is time from harvest to consumption, while other factors like price and being organic matter little. And it turns out Walmart (!) does better than grocery stores on getting the goods to you in time, while farmers markets can be great but have large variance.
This also suggests that you need to consume what you buy quickly, and that buying things not locally in season should be minimized. If you’re eating produce for its nutrients, then the dramatic declines in average value here should make you question that strategy, and they he say that on this front frozen produce does as well or better on net versus fresh. There are of course other reasons.
It also reinforces the frustration with our fascination over whether a given thing is ‘good for you’ or not. There’s essentially no way to raise kids without them latching onto this phrase, even if both parents know better. Whereas the actual situation is super complicated, and if you wanted to get it right you’d need to do a ton of research on your particular situation.
Are Vegetables a Scam?
My guess is Mu. It would be misleading to say either they were or were not a scam.
Aella: I think vegetables might be a scam. I hate them, and recently stopped trying to make myself eat them, and I feel fine. No issues. Life goes on; I am vegetable-free and slightly happier.
Rick the Tech Dad: Have you ever tried some of the fancier stuff? High quality Brussels sprouts cooked in maple syrup with bacon? Sweet Heirloom carrots in a sugar glaze? Chinese broccoli in cheese sauce?
Aella: Carrots are fine. The rest is just trying to disguise terrible food by smothering it in good food.
I have been mostly ‘vegetable-and-fruit-free’ for over 30 years, because:
If I try to eat most vegetables or fruits of any substantial size, my brain decides that what I am consuming is Not Food, and this causes me to increasingly gag with the size and texture of the object involved.
To the extent I do manage to consume such items in spite of this issue, in most cases those objects bring me no joy at all.
When they do bring me any joy or even the absence of acute suffering, this usually requires smothering them such that most calories are coming from elsewhere.
I do get exposure from some sauces, but mostly not other sources.
This seems to be slowly improving over the last ~10 years, but very slowly.
I never noticed substantial ill-effects and I never got any cravings.
To the extent I did have substantial ill-effects, they were easily fixable.
The claims of big benefits or trouble seem based on correlations that could easily not be causal. Obviously if you lecture everyone that Responsible People Eat Crazy Amounts of Vegetables well beyond what most people enjoy, and also they fill up stomach space for very few calories and thus reduce overall caloric consumption, there’s going to be very positive correlations here.
All of nutrition is quirky at best, everyone is different and no one knows anything.
Proposed actions in response to the problem tend to be completely insane asks.
People will be like ‘we have these correlational studies so you should change your entire diet to things your body doesn’t tell you are good and that bring you zero joy.’
I mean, seriously, f*** that s***. No.
I do buy that people have various specific nutritional requirements, and that not eating vegetables and fruits means you risk having deficits in various places. The same is true of basically any exclusionary diet chosen for whatever reason, and especially true for e.g. vegans.
In practice, the only thing that seems to be an actual issue is fiber.
Government Food Labels Are Often Obvious Nonsense
Government assessments of what is healthy are rather insane on the regular, so this is not exactly news, but when Wagyu ground beef gets a D and Fruit Loops get a B, and McDonald’s fries get an A, you have a problem.
Yes, this is technically a ‘category based system’ but that only raises further questions. Does anyone think that will in practice help the average consumer?
I see why some galaxy brained official might think that what people need to know is how this specific source of ground beef compares to other sources of ground beef. Obviously that’s the information the customer needs to know, says this person. That person is fruit loops and needs to watch their plan come into contact with the enemy.
As with all nutritional and diet advice, this seems like a clear case of different things working differently for different people.
And I am confident Bryan is stat-maxing sleep and everything else in ways that might be actively unhealthy.
It is however worth noticing that the following are at least sometimes true, for some people:
Bryan Johnson:
Eating too close to bedtime increases how long you're awake at night. This leads you to wanting to stay in bed longer to feel rested.
High fat intake before bed can lower sleep efficiency and cause a longer time to fall asleep. Late-night eating is also associated with reduced fatty acid oxidation (body is less efficient at breaking down fats during sleep). Also can cause weight gain and potentially obesity if eating patterns are chronic.
Consuming large meals or certain foods (spicy or high-fat foods) before bed can cause digestive issues like heartburn, which can disrupt sleep.
Eating late at night can interfere with your circadian rhythm, negatively effecting sleep patterns.
Eating late is asking the body to do two things at the same time: digest food and run sleep processes. This creates a body traffic jam.
Eating late can increase plasma cortisol levels, a stress hormone that can further affect metabolism and sleep quality.
What to do:
Experiment with eating earlier. Start with your last meal of the day 2 hours before bed and then try to 3, 4, 5, and 6 hours.
Experiment with eating different foods and build intuition. For me, things like pasta, pizza and alcohol are guaranteed to wreck my sleep. If I eat steamed veggies or something similarly light hours before bed sometimes, I usually don't see any negative effects.
Measure your resting heart rate before bed. After years of working to master high quality sleep, my RHR before bed is the single strongest predictor of whether I'll get high quality or low quality sleep. Eating earlier will lower your RHR at bedtime.
If you're out late with friends or family, feel free to eat for the social occasion. Just try to light foods lightly.
I’ve run a natural version of this experiment, because my metabolism is so slow that I don’t ever eat three meals in a day. For many years I almost never ate after 2pm. For the most recent 15 years or so, I’ll eat dinner on Fridays with the family, and maybe twice a month on other days, and that’s it.
When I first wrote this section, I had not noticed a tendency to have worse sleep on Fridays, with the caveat that this still represents a minimum of about four hours before bed anyway since we rarely eat later than 6pm.
Since then, I have paid more attention, and I have noticed the pattern. Yes, on days that I eat lunch rather than dinner, or I eat neither, I tend to sleep better, in a modest but noticeable way.
I have never understood why you would want to eat dinner at 8pm or 9pm in any case - you’ve gone hungry the whole day, and now when you’re not you don’t get to enjoy that for long. Why play so badly?
The other tendency is that if you eat quite a lot, it can knock you out, see Thanksgiving. Is that also making your sleep worse? That’s not how I’d instinctively think of it, but I can see that point of view.
What about the other swords in the picture?
Screen time has never bothered me, including directly before sleep. Indeed, watching television is my preferred wind-down activity for going to sleep. Overall I get tons of screen time and I don’t think it matters for this.
I never drink alcohol so I don’t have any data on that one.
I never drink large amounts of caffeine either, so this doesn’t matter much either.
Healthier food, and less junk food, are subjective descriptions, with ‘less sugar’ being similar but better defined. I don’t see a large enough effect to worry about this until the point where I’m getting other signals that I’ve eaten too much sugar or other junk food. At which point, yes, there’s a noticeable effect, but I should almost never be doing that anyway.
Going to bed early is great… when it works. But if you’re not ready, it won’t work. Mostly I find it’s more important to not stay up too late.
But also none of these effects are so big that you should be absolutist about it all.
We now studied the Total energy expenditure (TEE) of 4799 individuals in Europe and the USA between the late 1980s and 2018 using the IAEA DLW database. We show there has been a significant decline in adjusted TEE over this interval of about 7.7% in males and 5.6% in females.
We are currently expending about 220 kcal/d less for males and 122 kcal/d less for females than people of our age and body composition were in the late 1980s. These changes are sufficient to explain the obesity epidemic in the USA.
What’s the best way to exercise and get in shape? Matt Yglesias points out that those who are most fit tend to be exercise enjoyers, the way he enjoys writing takes, whereas he and many others hate exercising. Which means if you start an exercise plan, you’ll probably fail. And indeed, I’ve started many exercise plans, and they’ve predictably almost all failed, because I hated doing them and couldn’t find anything I liked.
Ultimately what did work were the times I managed to finally figure out how to de facto be an exercise enjoyer and want to do it. A lot of that was finding something where the benefits were tangible enough to be motivating, but also other things, like being able to do it at home while watching television.
Unlike how I lost the weight, this one I do think mostly generalizes, and you really do need to just find a way to hack into enjoying yourself.
Diane Yap: I know this guy, SWE manager at a big tech company, Princeton grad. Recently broke up with a long term gf. His idea on how to get back in the dating market? Go to the gym and build more muscles. Sigh. I gave him a pep talk and convinced him that the girls for which that would make a difference aren't worth his time anyway.
ofir geller: it can give him confidence which helps with almost all women.
Diane Yap: Ah, well if that's the goal I can do that with words and save him some time.
Andrew Rettek: The first year or two of muscle building definitely improves your attractiveness. By the time you're into year 5+ the returns on sexiness slow down or go negative across the whole population.
As someone who is half a year into muscle building for health, yes it quite obviously makes you more attractive and helps you feel confident and sexy and that all helps you a lot on the dating market, and also in general.
The in general part is most important.
Whenever someone finally does start lifting heavy things in some form, or even things like walking more, there is essentially universal self-reporting that the returns are insanely great. Almost everyone reports feeling better, and usually also looking better, thinking better and performing better in various ways.
It’s not a More Dakka situation, because the optimal amount for most people does not seem crazy high. It does seem like not a hard decision.
Exercise and weight training is the universal miracle drug. It’s insane to talk someone out of it. But yes, like anything else there are diminishing returns and you can overdose, and the people most obsessed with it do overdose and it actively backfires, so don’t go nuts. That seems totally obvious.
A Note on Alcohol
A plurality of Americans (45%) now correctly believe alcohol in moderation is bad for your health, versus 43% that think it makes no difference and 8% that think it is good.
It was always such a scam telling people that they needed to drink ‘for their health.’
I am not saying that there are zero situations in which it is correct to drink alcohol.
I would however say that if you think it falls under the classification of: If drinking seems like a good idea, it probably isn’t, even after accounting for this rule.
Focus Only On What Matters
I call that Finkel’s Law. It applies here as much as anywhere.
My basic model is: Exercise and finding ways to actually do it matters. Finding a way to eat a reasonable amount without driving yourself crazy or taking the joy out of life, whether or not that involves Ozempic or another similar drug, matters, and avoiding acute deficits matters. Getting reasonable sleep matters. A lot of the details after that? They mostly don’t matter.
But you should experiment, be empirical, and observe what works for you in particular.
> Diane Yap: I know this guy, SWE manager at a big tech company, Princeton grad. Recently broke up with a long term gf. His idea on how to get back in the dating market? Go to the gym and build more muscles. Sigh. I gave him a pep talk and convinced him that the girls for which that would make a difference aren't worth his time anyway.
Reminder that if you are a man, never take dating advice from a woman.
Regarding the vegetables thing, I do blame Anglos' retarded food culture for the fact that you + Aella etc. don't like veg. In countries with a healthy food culture, vegetables are just an integral part of nice food - curries, spicy hot pots, tasty soups etc. In Anglo food culture, it's mostly if you want a "healthy option", more commonly eaten as salads or joyless boiled green things on the side.
So I think you're missing out if you can't appreciate veg. Even if you think there's something superficially unpleasant about eating veg, to misquote Zvi from two weeks ago, "the failure to experience the sublime in things that people traditionally think are not [delicious] is a Skill Issue",
But, as a big veg lover myself, I'm not actually sure whether it's healthier or not to eat loads of veg. I like liking vegetables, because I like eating (both the social and hedonic aspect), and veg bulks up a meal and extends eating time by 2x or 3x. This probably means I eat slightly less healthily for some meals, because add more fatty/salty sauce to cover the veg appropriately etc. But I'm reasonably effortlessly slim and fit, so take as you will.
If you want to skip the backstory and just get to the instructions, click here.
If you’re a paid subscriber and you want to learn about more effective options than Ozempic or about sources with verified quality, click here.
Wegovy (Ozempic, Semaglutide)1 was found to be extremely effective for safely achieving weight loss and subsequently approved for its treatment in 2021. Since then, it’s enjoyed a level of popularity like no other drug before it. In fact, the whole class of drugs—GLP-1 receptor agonists, or just GLP-1s—has enjoyed skyrocketing popularity. In early 2024, the Kaiser Family Foundation polled Americans about their GLP-1 drug usage and reported that one-in-eight had used the drugs at least once.
With that popularity came shortages: manufacturers simply could not keep up with Americans’ demand for safe and effective weight loss medication. When the FDA declared that there were GLP-1 shortages, that meant that millions of Americans made their first contact with compounding pharmacies, because a shortage meant these pharmacies were cleared to produce and sell their own preparations of these drugs.
When compounding pharmacies started selling their own Ozempic, they definitely alleviated the shortages, and they worked to make the drugs far more available than they would be otherwise, in two main ways:
Several of these pharmacies provided a process for would-be users to obtain prescriptions for GLP-1 drugs. It’s an open secret that this process was more lenient than the typical prescription process that takes place at a doctor’s office.
Compounding pharmacies offered much lower costs for many potential GLP-1 users because insurance coverage of GLP-1 drugs is spotty. These users would have had to choose between paying upwards of $1,000 per month or $300 via compounding pharmacies. At the former price, the drugs were often unaffordable.
But access doesn’t have to be cut off. Plenty of people have discovered that GLP-1 drugs are easy to prepare yourself. While I legally cannot and I do not recommend doing that, those who want to can follow the steps below to accomplish that goal.
How To Get Very Cheap Ozempic
Step one in getting very cheap Ozempic is to find a peptide source. There are tons of these online and you can find them by Googling things like “buy Ozempic peptide”. Lots of reliable sources come up on the first page with that search, but if you want to see my preferred source, go to the section after this one. A bottle of Ozempic peptide looks like this:
Using my preferred source, you get 31 weeks of Ozempic using the typical dosing schedule for $501.5 total, or $64.71 per month. After getting to week 17, the per-month price rises to $96.3 per month (assuming a month = four weeks) because you’re using 2.4 mg per week—about one-third what compounding pharmacies were selling for. Do note: It is possible to do better than this price (i.e., $19 per month), but the purity guarantees doing that are inferior, so I cannot say I ‘prefer’ or ‘recommend’ that in any sense. Adventurous people can still choose to do that if they so wish! [Update: My ‘preferred’ source linked below sells Ozempic for $15.47/month.]
Once you’ve found a source and ordered your peptides, let’s talk storage. Before reconstitution, I recommend keeping them in the freezer. This extends their shelf life from months to years. After reconstitution, do not freeze them, but do refrigerate them when you’re not actively trying to use them. If your refrigerator is so cold that it freezes a reconstituted peptide, you’re making a mistake. Now to be clear, you do not need to keep them refrigerated when you’re drawing from your vials either, refrigeration is just for when you’re not preparing an injection.
With peptides in hand, you’ll still need to order a few more things before you can inject yourself. Luckily, those things are cheap, legal, and readily available. You’ll need:
Bacteriostatic water. This is crucial for preparing your Ozempic and you can get it on Amazon, or often enough, from peptide sources themselves. Bacteriostatic water can be kept at room temperature until opened, whereafter it should be refrigerated.
Sterile syringes. These are going to be used for transporting bacteriostatic water and Ozempic. They are very cheaply available in bulk on Amazon, Aliexpress, and through many other online retailers. I recommend getting 1 mL syringes for pulling from your vials and injecting and 3 mL syringes for putting bacteriostatic water in.
Sterile needles. These are going to be used for penetrating your bottle of Ozempic, your bottle of bacteriostatic water, and your fat butt2 (or stomach, or arms, or wherever you feel most comfortable injecting). They’re readily available on Amazon, Aliexpress, and elsewhere, like the other ingredients are. I recommend 4mm needles at 30 or 32 gauge for adding bacteriostatic water to your Ozempic and for pulling Ozempic from your vials, and 34 gauge needles (higher gauge = thinner needle) for injecting, but the size of needles you use is up to your personal preference.
Sterile swabs. Any old alcohol swabs will tend to do. You can get these at Walmart and other superstores, on Amazon, Aliexpress, and in so many other places. If you’re the sort of person to own a first aid kit (which you should be), then you probably already have a lot of these in your home. If not, just buy them; they’re extremely cheap.
And that’s all you’ll need. If you’re a judicious shopper, it should cost you about $40 to get all of this in sufficient quantities to go for a year or more. If you’re not good at finding good prices, I could see someone paying $60 for this or more if they’re buying very large quantities of this stuff for whatever reason. Do your shopping right and this should add no more than $3 per month to your Ozempic bill.
Now that you’ve acquired your peptides and all the tools you need, it’s time to reconstitute your peptide. This simply means turning them from a crystallized form to a liquid one that you can inject. You start by getting out one of your vials of your Ozempic peptide and another vial of your bacteriostatic water. They will have caps on them, like the red cap in the illustration below. Take those off. Do not take off the metal cap with the gray plastic on top of it. That’s the sterile barrier.
Now prepare a syringe. Grab one of your syringes and pull back the quantity of air equal to the amount of bacteriostatic water you want to pull from your bottle. This amount will vary depending on how much of the peptide is in your vials, but for the formulation I recommend, I supply quantities in the section below. This information will always be trivial to calculate, but if you’re having trouble, Google it. Put a needle for drawing out bacteriostatic water on it, and grab an alcohol swab. You’re going to use the alcohol swab on your bacteriostatic water vial’s lid before you put the needle through the bottle’s gray plastic part on the lid. Next, push in the air and draw back the required amount of water.
Now that you have your bacteriostatic water drawn into your syringe, take the needle out and use a fresh alcohol swab on the vial for your peptide. Put in the needle with the bacteriostatic water and inject the water before removing the needle and disposing of it and the syringe safely, meaning not letting a needle just lie loose. If you have stable hands, put the cap back on the needle before disposal; if you do not, then don’t bother with recapping it, because you might prick yourself, and that can suck. To dispose of a needle safely, place it in hard-sided container with a lid, such as a food storage box or an empty laundry detergent canister.
Wait a moment until there are no more chunks in your bottle, at most gently swishing around your peptide. Once you just see a clear liquid, you have reconstituted Ozempic! Now it’s time to get it in your body.
Take a fresh syringe and needle and pull back the quantity of air equal to the quantity of Ozempic you want to draw, swab down the top of the vial (do this each time you need to prick it), put your needle on your syringe, and pierce through the top of the vial and draw the quantity of Ozempic you want. Once you’re done, pull out the needle and dispose of it safely, before putting on a fresh needle. Now onto injection.
When you have a prepared needle and syringe, you just need to alcohol swab your injection site thoroughly and put the needle in and inject. It’s that simple, but if you’re not familiar with how to do this, just look it up online. There are tons of video guides to do this. The injection site can be any appropriate subcutaneous fat injection site, but I recommend injecting into belly fat, because for most people, that’s the easiest way to do this. If you’re lean enough that it’s not the easiest site for you, then search around for an appropriate site.
And that’s all it takes! Go store the remaining part of your vial, and you’re done. If you did everything right, you just prepared and injected cheap, high-quality, homemade Ozempic. Congratulations on the biohacking.
Ozempic Is Not The Top GLP-1 Drug
If better priced sources than the ones linked below emerge, I will provide links to those as soon as I’m aware of them.
Ozempic produces staggering weight loss. Compared to a lifestyle intervention and a placebo injection, a lifestyle intervention plus Ozempic3 led to a 15% reduction in bodyweight in this trial. Other trials show similar results.
Tirzepatide is, for all intents and purposes, Ozempic Plus. It has a similar primary GLP-1 receptor agonist-based method of action, but it also adds another ingredient: GIP, or gastric inhibitory polypeptide, a weak inhibitor of gastric acid secretion and another insulin secretion stimulator. This makes Tirzepatide more effective, but adding an ingredient does increase the a priori odds of side effects. Anecdotally, I have known two women who had mental side effects on Tirzepatide that they did not have when they used Ozempic. On the other hand, people have told me that their memory improved with GIP, which was actually a predicted side effect based on how it works.
But Tirzepatide is not the top GLP-1 drug. That title currently goes to Retatrutide, which is basically Tirzepatide Plus. Like Tirzepatide, Retatrutide contains a GLP-1 receptor agonist, GIP, and it also adds in glucagon, resulting in some interesting effects that are particularly pronounced in the liver. In fact, one phase 2 trial found that Retatrutide has excellent effects on markers of liver health.
And why shouldn’t it be? Retatrutide is lean mass sparing, meaning that what loss happens has even more to do with fat than occurs with Ozempic or Tirzepatide. Retatrutide is also metabolism boosting and metabolism sparing. Where weight loss tends to lead to decreased metabolism, becoming harder and harder as it continues, Retatrutide blunts that effect. In one particularly revealing experiment, mice were injected with Retatrutide or nothing and subjected to the same diets and temperatures. The Retatrutide mice lost 35% of their body weight while the matched mice lost just 20%. When Retatrutide-treated mice were treated with glucagon antibody antagonists, this added weight loss effect stopped. Exploration reveals that Retatrutide increases fat mass reduction through increased lipid oxidation, supplementing energy levels, leading to maintained locomotor activity. Perhaps this is also related to why it seems to reduce visceral (belly) fat so selectively.
The wonders of this drug go on and on. It really is incredible, and anecdotally, people report to me that it’s more tolerable than both Tirzepatide and Ozempic. I don’t know if that will hold up, but I will note that the trial results suggest limited side effects. [Edit: Retatrutide does show a cardiac safety signal. This may be due to the added glucagon, but that’s not clear quite yet. This is not worth worrying too much about unless you have a prior history of cardiac issues.]
To obtain Retatrutide, I would (if I were offering this advice) recommend buying from Solution Peptides. They are the source I am currently saying I would recommend because they:
Have verified high quality products. Their product purity is very high.
Have the lowest prices I’ve found. With the addition of discount code “heather15” at checkout, orders are marked another 15% off from their already competitive pricing. Usage of that code is how I achieved the $501.5 figure for Ozempic I mentioned earlier.
A 10-vial pack of Retatrutide can be obtained from this link. A 10-vial pack of Ozempic (Semaglutide) can be purchased from this link. This source also sells bacteriostatic water with pricing that is very competitive, even before applying the 15% discount code.
Nexaph. They are a source with an active community, frequent testing, and extremely good prices. Their Easter rate for Retatrutide is 240 mg for $350, which for most Americans, nets out to about $367.50 after shipping and handling. Normally, their rate for the same quantity is $550, which is still an incredible deal that stacks up well compared to other sources that have quality testing going on. Without the 15% off deal from my previous recommended source, Solution Peptides, the $350 deal is 84.5% better, and at $550 for the same amount, it’s 75.8% better.
Nexaph’s price for Semaglutide is even more outrageously low. They’re selling a 100mg kit consisting of 10 10mg vials for $170. At a 2.4mg weekly dose, that nets out to $4.08 dollars per week for almost 42 weeks. I no longer recommend Nexaph. They set up an online community, the community demanded overfilling vials beyond their labeled quantities, and reports have come out showing that they supply much more Retatrutide, Tirzepatide, and Semaglutide than their labeled dosages. For example, in a recent batch of Retatrutide, they labeled the bottles as containing 24mg, but they contained 30-34mg. The product was completely pure, but providing too much means that the bottles cannot be trusted without everyone engaging in testing.
While this is unlikely to cause any meaningful level of harm beyond an upset stomach because of the excellent safety profile of these drugs, it’s still not trustworthy behavior, so I no longer recommend them. If you want more product than you think you’re buying and you’re OK with guesswork or sending off a test bottle or two, then Nexaph will still be fine for you.Now I really don’t recommend Nexaph. Their most recent batch ‘addressed’ the overfill issue by being slightly underfilled by about 10%, and it had subpar, 97.3% purity. I cannot in good conscience recommend them until they return to at least 99% purity. I realize purity issues are not entirely their fault, but I can see that this has a lot to do with rushing to meet demand. They will need to earn back trust.
Peptide Partners. This source is credible and is selling Retatrutide, Tirzepatide, and Semaglutide at reasonable prices. For Retatrutide, someone using a 4mg weekly dose would end up paying $41.60 per month at their prices, and if they were to use their Tirzepatide, they would end up paying $130.00 per month with a 15mg weekly dose. Their Semaglutide, on the other hand, only costs $18.20 per month at a 2.4mg weekly dose. [Edit: Peptide Partners reached out to give me a discount code for you all to use to get an additional 15% off of your order. The code is ScrewTariffs, and it’s applied in your cart. This drops the monthly prices for Retatrutide, Tirzepatide, and Semaglutide, respectively, to $35.36, $110.50, and $15.47 per month. Edit II: Peptide Partners also uses the 15% discount code doge. I want to reiterate that I like this source for their quality guarantees. For example, they use a domestic lab—TrustPointe in Michigan.]
May 31 update: My new and current recommendation is to vet sources using Finnrick. Finnrick compiles results for various sources and grades them based on purity of the product, the quantity relative to the labeled amount, and the presence of batch identifiers. If companies over- or underfill their vials, they’re penalized; if their product is less pure than desired, they’re penalized; if there are no batch identifiers, they’re penalized. This is a good way to do things. This does not grade on price, so I will continue providing price-based recommendations as well, but if those are not up to date, you can search for price information by clicking through sites reviewed by Finnrick.
June 17 update: If you want a strong quality guarantee with a somewhat higher price, I recommend looking through the top of Finnrick’s list. Solution Peptides is also still good, and their prices remain reasonable, albeit not pack-leading.
I have no financial interest in these sources (original post source: Solution Peptides; second post source: Nexaph; third post source: Peptide Partners; fourth post source: Pure Rawz; fifth post source: Finnrick’s list), am not using any sort of referral link, do not benefit from any discount codes, and am not profiting from this in the slightest. I am not even recommending this be done in the first place. If another source comes up that is priced better, with as much data to indicate its product quality, I will recommend that source instead. And remember, sources can always go from offering good product to bad product in the blink of an eye; I am not assuming responsibility for product quality changes.
If you purchase a 10mg vial of Retatrutide from any source, like Solution Peptides, the mixing instructions are simple. Just add 2mL of bacteriostatic water for reconstitution, and then if you want to inject a typical dose that I’ve seen people use with high efficacy, inject 0.4mL for 2mg a week. If you elect to use their cheap Ozempic instead, the amount of bacteriostatic water to add is also 2mL.
Titration is optional, but important to maximize the benefits of GLP-1RAs while keeping their side effects in check. People who fail to step up their dosages cautiously risk side effects that range from annoying to serious. Of course, stepping up dosages at all is optional; no one is being compelled to increase their dosage from a bare minimum quantity. Ultimately, the choice to do so is up to the user, and where they end up dosage-wise is a matter of personal discretion. People generally see larger effects at higher doses, with considerably diminishing effects outside of current dosage schedules.
In order to minimize side effects, semaglutide is prescribed with the following dosage schedule, reprinted from above:
Tirzepatide, on the other hand, is quite a different chemical, and its equivalent dosage schedule looks like this:
Retatrutide lacks an FDA approval at the moment. As a result, there is no published recommended dosage schedule. Following in the style of the tirzepatide chart, this is what I’ve gathered to be the likely dosage schedule for retatrutide when it’s finally released. This chart is based on testimony from trial participants and long-time users. It does not reflect a recommendation so much as what I believe to be the likely dosage schedule.
This dosage schedule is speculative, and when an official one is released, I will post an update here. Individuals who are lighter, or often enough just female, may prefer starting with 1mg. From surveying users, I’ve found that often makes sense and 2mg is too heavy a start for some. Do what works for you, surveil trials to see how people react to different dosages if you feel you need to, and most importantly, do what feels right. At the end of the day, if a certain dosage is too much for you, then dialing it back might be your best move. I hope this dosage schedule chart can be informative.
August 24 2025 Update: Slow Titration and Side Effects
Most of the popularly-hyped side effects of GLP-1RAs are not real (e.g., muscle-wasting, pancreatitis, colorectal and thyroid cancer, major adverse cardiovascular events); are incredibly rare and tied to preexisting conditions (e.g., proliferative retinopathy)4 ; or are exaggerated to high heaven (e.g., gastrointestinal side effects). The most common side effects of GLP-1RAs fit in the last category and they include things like nausea, vomiting, diarrhea, constipation, and delayed gastric emptying (otherwise known as gastroparesis). But, these side effects are:
Almost always non-severe, they might annoy, but they rarely cause serious harm;
Usually fleeting, they come and go fast;
Considerably population-specific;
Rarer on tirzepatide and retatrutide than with semaglutide;
Typically avoidable through slow titration.
These factors are incredibly important, and I’ve made sure to mention them from time-to-time for an important reason: I hate the idea of people irrationally fearing medications that could greatly improve their lives. It just won’t do for people to be afraid of something that could, at once, extend their lifespan, improve their healthspan, and bolster the quality of their life in a variety of ways having to do with aesthetics. So, below, you’ll find a brief review, and then I’ll get into concrete strategies to avoid side effects.
Secondly, as many trials have shown, side effects fade out. The quotation above suggests this tends to no longer be an issue after dose escalation (i.e., titration), and that is true. With gastroparesis, both in trials and in preclinical studies, the same is true: it tends to go away fairly quickly. Consider the result of this head-to-head trial comparing semaglutide and tirzepatide:
Aronne et al. 2025, Figure S9A
Moreover, these gastrointestinal side effects are reactive, meaning that they occur based on the things you do while on the drugs. I’ll return to this below.
A more important thing to note about diabetic and nondiabetic use of these drugs is that rare, extreme side effects are practically only seen among diabetics. The most common examples of this in the press are microvascular harms—that is, damage to small vessels, and particularly in the eyes. If you check Footnote 3 and what it’s a comment on, you’ll see an example of this. Basically, diabetics can fare poorly with GLP-1RAs for the same reason that they fare poorly with intensive insulin therapies: getting their HbA1c (blood sugar) under control too quickly shocks the body and can cause issues. For diabetics who are already under control, or people who are nondiabetic, this should not be an issue, so there’s no need to fret over it.
Fourth, newer drugs tend to come with fewer side effects and greater efficacy. Older GLP-1RAs like exenatide and liraglutide cause more distress to patients, require greater numbers of injections (unless you’re on a long-acting version), and tend to work worse for glycemic control and weight loss. This is even true comparing semaglutide (as a reminder, that’s the active ingredient in Ozempic/Wegovy) to tirzepatide (the active ingredient in Mounjaro/Zepbound). Consider the rates of vomiting and nausea in comparable trials for both drugs:
Tirzepatide gives a walloping to semaglutide. It is both a more effective drug and a drug with superior safety: fewer and less severe side effects! This is driven by its five-times weaker GLP-1R agonism that seems to happen due to co-occurring GIPR signaling in the hindbrain. This superior side effect profile is why, I’ve found, I can transition friends who struggle with gastrointestinal issues on semaglutide over to tirzepatide or retatrutide (which is broadly similar to tirzepatide in terms of its side effect profile) and see them succeed at substantially higher rates.
Here’s the part you might care more about: How can you lower rates of side effects?
Beyond choosing to use tirzepatide or retatrutide over semaglutide, the first thing to note here is that most side effects of a gastrointestinal nature are reactive. The longest term variety of interaction here is through failing to eat a healthful diet, causing constipation. Normally, with excessive food consumption, you might get enough fiber, for example, but after you cut back on eating, you might get far less, proportionally and totally, leading to blockage. The most important interaction for acute nausea, vomiting, and so on, is with binge eating and drinking. I’ve helped people to overcome issues with these drugs on several dozen occasions now, where the problem was nothing more than that they had a problem of eating beyond the point where they were full. If you eat or drink too much, you’ll feel sick on or off these drugs, it’s just that, off them, the threshold is a lot higher. Keep that in mind.
The second thing to note is that you can prevent most side effects with slow titration. Consider this result from a recent trial of semaglutide. Study the chart:
Eldor et al. 2025, Graphical Abstract
With a slower increase in dose compared to the typical titration schedule that I’ve shown above, people ended up with less than half the number of days feeling nauseous. That’s huge! This also replicates. For example, here’s a result for tirzepatide:
Further evaluation of [gastrointestinal adverse events, i.e., gastrointestinal side effects] incidence from the first onset data showed that the [adverse events] most probably to occurred following the first dose (4 or 2.5 mg), and the incidence and prevalence may have been reduced with lower starting doses… Also, smaller subsequent dose escalations were more probably associated with a lower incidence of the combined nausea, vomiting and/or diarrhoea [adverse events].
This replicated in other tirzepatide trials, like SURPASS-2:
The dose-escalation scheme in the current trial of the phase 3 SURPASS clinical program, which included a lower starting dose and slower dose escalation in smaller increments, was associated with a better gastrointestinal-related side-effect profile than the scheme in the phase 2 trial, which involved more rapid escalation. Gastrointestinal adverse events reported with tirzepatide and semaglutide were consistent with those that would be expected with the GLP-1 receptor agonist class and were mostly mild to moderate and occurred during the escalation period with both trial drugs.
This slower titration schedule led to fewer discontinuations, fewer total adverse events, and everything else you’d expect if people were hurting less. In the real world, the improved rates and severity of side effects with tirzepatide are associated with better adherence. This result holds up with other GLP-1RAs and with numerous other drugs as well.
So, struggling with side effects? Or worried about struggling with side effects? It’s simple: start small and go slow. Begin your dosing with a low dose and increase gradually. You may not lose weight as quickly with this approach, but you’ll eventually get there without the issue of side effects haunting your way up the dosing ladder. If the trial results are to be believed—and they should be—then you also won’t lose weight that much more slowly with slower titration, so don’t feel like you’re missing out by doing this.
One dosing schedule I’ve been trying out on subscribers involves having them start with 0.5 mg per week of retatrutide and then moving it up by just 0.25 mg per week, until they feel comfortable moving it up more rapidly. This seems to work incredibly, and has helped plenty of people who struggled with normal dosing schedules to actually stick with the drugs without a problem.5
What I encourage you to do, if your aim is avoiding side effects, returning to the drugs without side effects, reducing the extremity of side effects, or any combination or permutation thereof, is to go slow, and if something feels bad, pull back your dose, let it work, and up it again—only if you need to—at a later point. If you do this right, you can trivially use these drugs without meaningful side effects.
Another thing I’ve been trying has generated some more marginal improvements for people, and that is to get them to inject smaller amounts twice a week instead of one larger dose once a week. This helps to smooth over circulating levels throughout the week, which might help, but I’m not as confident in this conclusion quite yet, so I’ll leave this as a footnote until I’ve gathered more data.
Warning: This is an experiment log, I’m not advising you to start taking GLP-1s. I wish that there were more logs about people's experiences on peptides, so here's mine in case others find it helpful.
I started Retatrutide in late May. I wasn’t overweight; I wanted more energy and focus. My BMI was 20.3-20.5 so I could lose about 5-7% of body weight without falling into the underweight category; I wore size 2-6 in women’s clothing; I deadlifted and squatted 3x5 (3 sets of 5 reps) about 0.85x my bodyweight, and I could overhead press about 0.3x of it. I went with Retatrutide because some people said that it helped them with focus etc.
I'm at my most productive when I’m slightly hungry, but not extremely hungry. This feature proves good for morning work, and bad for any sort of afternoon work after lunch (I get productive again right before dinner, which is annoying for dinner plans and going to sleep at a reasonable hour because I can't sleep right after eating). I had my (fasting) blood sugar tested two years ago and it was in the normal range. I also wore a CGM and played around with meal sizes and amounts of sugar, but energy levels and blood sugar did not seem to correlate much. I have tried to eat high protein with low carb or low fat and neither works; the only thing that really worked was to eat meals that had less than 300 calories. Which is not very conducive if I didn’t have the time the previous week to meal prep, and I had to consciously eat when I didn’t feel super hungry so I wouldn’t still feel quite hungry after 300 calories.
I had gained about 17 pounds over three years in college, and I lost 10 of those during graduate school (I did rapidly lose 10 lbs over 6 weeks right out of college because of budget constraints but I immediately gained back 5 lbs when the constraints were relaxed. I eventually lost the 5 lbs in the second year of grad school). I could lose weight, but I also wasn't really trying to lose weight, if that makes sense.
Week 1-2
The typical dosing used in trials is 1 mg/week for the entirety, or 2 or 4 mg/week for 4 weeks and then staying on 4 mg/week for the rest of the trial, or titrating up to 8 or 12 mg/week. Most weight loss seemed to start around 4 mg.
I started at 0.5 mg/week, below any of the initial trial doses, but some forum users said that a lower dose would decrease the likelihood of side effects, and I was smaller than the typical Retatrutide user. I also had fairly bad side effects from some types of birth control, and I didn't want to risk having too much in my system and being in agony for a week.
During these two weeks, I would feel some semblance of hunger pangs, but they were extremely ignorable and in the background. My appetite mainly stayed the same, I think. I wore a CGM during the first week, and my blood sugar was far more stable, even when I'd eat something extremely sugary for lunch.
Focus/Productivity
I don't think I was more productive per se, it was slightly easier for me to focus on things like writing (compared to coding which has a tighter feedback loop). I wrote a non-zero amount, but also not as much as I would have liked. But the lack of writing is also confounded with conference deadlines; I stayed up until 2 am one night to finish some experiments. My twitter usage went down slightly.
Side effects
My sleep was definitely worse, I often would wake up a few hours before my normal wake time and fall back into some weird, troubled, dream-filled sleep. I felt tired in the mornings sometimes, but drinking electrolytes fixed it. I mostly stopped drinking caffeine in the mornings, and didn't get caffeine withdrawal (I have tried to quit previously and I would lead to headaches in the afternoon for the first few days).
My watch yelled at me for a lower HRV and higher resting stress, but that seems to a common side effect. My resting heart rate went up by 5 bpm.
In these two weeks, I didn’t really lose any weight, it just fluctuated within the normal range. The 7-day average at the end of the 2nd week was only 0.4% lower than my starting weight, which really rounds to zero (I actually gained 0.3 percentage points in the first week and then lost a bit more in the second week).
Week 3-4
Then I went up to 1mg/week.
My reasoning was something like, “I’m feeling all the side effects (higher heart rate, worse sleep, low HRV) and only some of the benefits (a tiny bit of focus), maybe I should start being on the actual starting dose to see if there are any effects.”
Focus/Productivity
Better focus kicked in after day 2 on 1 mg. I didn’t feel as tired before bed, but I’d often wake up tired until I drank electrolytes. My productivity went way up. I drafted an entire paper over the course of a week, including collecting and processing 75% of the data that I needed. This could be caused by stress because I really needed to get this thing done, but I have not been able to summon this type of productivity even during college (when I was arguably the most productive). I used to feel useless after 9 pm, and I haven't been able to wake up before 6 am to make use of the morning since third year of grad school, and now I can work between 9-11 pm. My twitter usage has gone down by about a third to about a half; I was writing a lot more than the past. Over the last year, I constantly had "oh I need to write" hanging over my head, but seldom would successfully put words on a page.
Hunger pangs were mostly gone; I could eat a meal a day and feel full, so I was roughly only eating two meals. I think there was a day where I only ate 200 calories and wondered why I was hungry in the evening. The hunger suppression was unironically great for productivity and I had a steady stream of energy throughout the day. I was constantly in the “a little bit hungry” state but almost never in the “ravenously hungry” level, my happy zone for productive work.
Side effects
My watch continued to say that I didn’t sleep well, my HRV was low, and my exercise status was strained. My resting heart rate went up another 5 bpm (so 10 bpm higher than baseline). On the second week of 1 mg, I noticed that my heart rate went up higher much faster when climbing too. This means faster and easier warmups, but worse endurance when trying to finish a route. My lifts were about the same if not slightly heavier. I also sweated more.
Sometimes I’d eat at 8 or 9 pm, and this would cause acid reflux when I went to bed at 11 pm because Retatrutide slows down stomach emptying, and I’d still feel like there was a lot of food in my stomach. I could still eat normal-sized meals, but I didn't need as many normal-sized meals. I would sometimes eat something extremely sugary and not feel the sugar crash afterwards, but I don’t particularly crave sugary things anymore.
The rate of weight loss was the highest in these two weeks. My 7-day average at the end of Week 4 was slightly under 3% of original weight.
Week 5
Focus/Productivity
I worked fairly hard at the beginning of the week. I hit a major milestone in getting the paper done, but only had a week until the next deadline. I hit the second deadline on day 4.
On day 5, I crashed. I didn’t sleep more than usual, but my bandwidth significantly decreased. I didn’t feel like doing anything. This is likely caused by a combination of several things: I was on the last week of birth control where the hormones are significantly reduced (starting on day 2 of this week), I hit relevant deadlines about which I was extremely stressed for 2 weeks on day 5, and some other life stress right after too. I also suspect that I spent more time in the “ravenously hungry” zone because I felt hungry often but would ignore it (because I didn’t feel like doing anything); the hunger pangs would go away and I’d just be as tired as before. My twitter use went up at the end of the week, but it also goes up when I’m feeling dull in general.
Side effects
I vomited on day 3 after exercising, because I had a protein bar too close to exercising (I don't recall vomiting before, but I also don't usually have a snack before climbing/lifting). I did deadlift 3x5 my body weight, up from 0.85x when I started this experiment.
My period also skipped, because of the rapid weight loss (this happened the summer I lost 10 lbs in 6 weeks naturally too).
I almost didn’t take the 6th dose and ended up delaying it by a day because I felt so tired, but I think I was physically more tired without Retatrutide because I was WAY more tired on day 8. This was partially intentional, partially I was too tired in the evening of the 7th day to think about injecting (last week, I used the same needle for drawing bacteriostatic water and injecting because I was spacey). By the evening of the 7th day, I felt quite tired and sluggish. On the morning of the 8th day, I felt extremely tired and almost missed work and I was like “okay this needs to stop.” Maybe Retatrutide just allows you to function better without enough food. I was eating roughly one meal and one snack.
I considered titrating down this week, but I wanted to see if the tiredness was entirely from external factors or due to Retatrutide, so I continued at the same dose.
I lost about another 1 percentage point this week, so 4.1% total.
Week 6
I think most of the physical tiredness is from the type of birth-control I’m taking; the hormone-free week causes a crash in hormones, potentially leading to tiredness according to o3. After two days on a new pack, the physical tiredness went away.
I maybe was even slightly higher energy because I went climbing twice in the first half of the week and did a fun physical arcade evening with friends. But mentally I was still quite tired. It was rough getting me to do things; I went climbing multiple times because I wanted the silence in my head after physical exertion. I finally could squat 1x body weight for 3x5 too.
I lost about another percentage point of original weight, so about 5.3% total.
Week 7
I decided to titrate up very slightly to 1.5 mg to see if it would deal with the mental tiredness. I shouldn’t have titrated up in hindsight.
Focus/Productivity
After day 2, I had really strong lack of motivation to do anything. I’d stay in bed for hours after waking up and didn’t want to get out of bed; I didn’t want to go to sleep at night because that meant a new day. Not sure if this was due to uncertainty around work, dislike of my work location (we moved co-working spaces into a larger shared space), low-grade stress about paper edits, lack of protein, or some third thing.
Side effects
I also really became *not* hungry at all when I physically felt hunger. I would not want to eat when my stomach was clearly empty and I should eat something. I typically ate things that I craved/wanted to eat, and earlier in the week I had issues with eating more than 200-300 calories in a meal. I ended up snacking on crackers a good bit this week.
I barely ate at all on 3rd day and that really messed up the 4th day because I felt very lightheaded in the morning but also nauseous when I had breakfast. I think I had some honey which helped with the lightheadedness and then had yogurt. But my stomach hurt for a bit and then subsided. At the end of the week, appetite suppression was still pretty strong and I felt like I couldn’t really eat normal-sized meals (equivalent of the previous week on day 2-3).
I’m now squarely in pre-college weight, lift 1x body weight, went up a climbing grade (this is likely just a function of time and climbing experience), probably lost some muscle but likely lost more fat because my proportions are still the same, just a bit smaller. I still wore the same clothes. Some did fit better, though.
I lost about 1.2 percentage points this week so I've lost 6.5% of original body weight so far.
Week 8
I really should have titrated down to 1 mg this week.
Focus/Productivity
Usually I feel a little tired but more focused after injecting, but I already was feeling somewhat uninterested in doing things, and it didn’t get better on day 2. I had to get paper edits done this week. This was pretty bad because I spent a good amount of time fighting myself to get work done.
I finally summoned up enough willpower to force myself to get this done on day 3 (I’m sorry Cate Hall, I know you disagree with this definition).
I hit the final deadline on day 5!
Side effects
I vomited this week after going on a walk and eating a babka (which isn’t that much food?!) on day 3.
The most pressing thing done, I think I can conclude this experiment. I’m at a point where I shouldn’t be losing that much more weight. I often feel more low energy than usual on day 7, so I’ll try to titrate down instead of stopping cold turkey.
I've lost about 7.7% of original weight now.
Week 9
I injected 1 mg this week; I didn’t realize how I mostly had gotten used to the lack of interest in doing things. I suddenly had motivation to do things again. I also spent less time on twitter this week compared to last week.
My appetite was still mostly gone, but I think I ate slightly more. I started eating breakfast (yogurt with chia seeds and hemp seeds), but I don’t know if this is because I regularly would skip dinner or the dosage was lower. But the hunger was comfortable—1.5 mg felt too strong where I would be hungry but not crave any food.
I still lost like 0.8 percentage points this week, so I've lost 8.5% of original weight so far.
I think I'll stop taking Retatrutide: my focus is slightly better, but my resting heart rate is close to 15 bpm higher than when I started, I would prefer to not sweat as much or have my heart rate spike as high during exercise. I would also like to get a good night of sleep again. I'm not sure if I'd have finished my dissertation this summer without Retatrutide, but I (hopefully) will be writing more code and fewer papers.
Things that didn’t really fit into weekly reports:
Here's a graph of how my BMI changed—I weighed in almost every morning, and my weight would end to tick up on the 5th or 6th day.
BMI trend throughout the experiment
I think I became slightly more forgetful/absent-minded because I misplaced items more frequently over the span of this experiment (thankfully I found most of them but some never turned up again). I typically don’t lose things; I think I've only lost one thing in the past year.
The amount I spent on food didn’t change because I already eat fairly frugally, if anything it went up as I ended up eating out more (mostly because I had more specific food cravings). If I was hungry enough, I’d eat anything but Retatrutide seemed to reduce that ability. I also did throw out more food because it went bad in the fridge.
Sarah Constantin said that she felt sleepy within 24 hours of the Ozempic shot; I actually felt quite alert and energetic right after an injection and moved my shots to the morning so I wouldn't have to consciously try to fall asleep.
Alcohol was strange. I had two standard drinks in one nights and felt hungover within three hours and still felt hungover in the morning. Before Retatrutide, I had never felt hungover in the morning (even after 3+ drinks), and I'd get a headache within an hour or so if I didn't drink enough water, and was fixable with water consumption. This time, I also didn't really feel a buzz when drinking alcohol, maybe something to do with the slower digestion on Retatrutide. I understand why alcoholics quit alcohol on GLP-1s, it's no longer fun anymore.
I exercised more over the course of this experiment than in the past, partially because I didn't want to lose muscle and partially because I got a smartwatch that would tell me nudge me to exercise (it's fun to see number go up in training load, for example).
My allergies towards dust weren't as bad as usual (I typically react to something in old houses and old furniture). I can't tell if this is due to weather changes or Retratrutide.
I suspect that the productivity benefits went away because I wasn't eating enough, and it takes a few weeks for your body to run out of fuel. I wish that I had tracked my food intake, because I was really tired on 1.5 mg and I definitely wasn't eating enough food.
\ No newline at end of file
diff --git a/docs/sources/www-lesswrong-com__posts-mlvek6a9g86enhjqh-30-days-of-retatrutide__b6d5765e5f.html b/docs/sources/www-lesswrong-com__posts-mlvek6a9g86enhjqh-30-days-of-retatrutide__b6d5765e5f.html
new file mode 100644
index 0000000..0562fa1
--- /dev/null
+++ b/docs/sources/www-lesswrong-com__posts-mlvek6a9g86enhjqh-30-days-of-retatrutide__b6d5765e5f.html
@@ -0,0 +1,38 @@
+
+
+
+
+
+
I've had trouble maintaining my weight since high school. If I eat "normally", I slowly gain weight, and if I eat nothing but a specific potato casserole, I slowly lose weight.
Recently, I hit a new high-record weight and decided it was finally time to do something more serious about it, so for the last month I've been taking the standard CICO diet advice. I finally realized that I should eat healthier, and eat significantly less. I work out slightly more. I cut out most high-fat foods and became strict about not eating after 6 pm.
Anyway, this is a post about my experience with retatrutide.
This is not a how-to article, so I'm not going to talk about where to get peptides or how to safely use them. See this article if you're into that sort of thing.
The Experiment
Retatrutide is a GLP-1 agonist similar to semaglutide (Ozempic), but which seems to cause more rapid weight less.
It isn't FDA-approved yet, but you can buy it for experimental purposes. I forgot to pre-register my experiment, but my hypothesis was that if I took 2 mg of retatrutide per week, I would lose weight.
I also failed to register this experiment with an IRB. My doctor told me that losing weight would improve several of my health conditions, but GLP-1 drugs are only indicated with a BMI 0.5 units higher. The standard of care is to not treat the underlying condition and to instead take a fistful of drugs every morning.
So, I guess my experiment was highly unethical. Luckily it was privately funded and the subject is unlikely to sue me.
Effects
For a few days after my first injection, pretty much all food repelled me. I tried to take 50 g of protein powder every day to limit muscle loss, but found it very difficult to stomach.
Food has become less repellent over time, and I mostly get through my protein powder now, but I still find it hard to eat more than 2/3rds of what I used to.
In terms of Axes of Hunger, I have much less of an appetite, sometimes experience minor / easily ignored hunger pangs, and don't seem to experience much emotional distraction from being hungry. I intellectually know when I should probably eat a meal, but can trivially ignore it if I'm busy and want to blog more.
I also find fatty food and alcohol much less tempting, although this might be because they exacerbate the side effects.
Over the first 30 days, I lost about 10 lbs and went down one belt size.
I was losing weight so fast initially that it was actually kind of concerning, so I forced myself to eat more. I assume the rapid weight loss was glycogen ("water weight"), since I still don't eat very much but weight loss has dropped to a less-concerning 1.5 lbs per week.
Side Effects
Muscle Loss?
I did some basic workouts to try to prevent muscle loss, including biking to work (3 days per week), a relatively hard 2 hour hike (once per week), two sets of ~15 pushups, and as many sets of 1-3 pullups as I remembered to do.
I don't track my workouts very well, and I don't have any objective lean mass data, but:
I do around the same number of pushups as I could 30 days ago.
I can do more pullups (probably because they're 10% easier).
Biking feels about the same.
Hiking is terrible, but I think that's because of my heart rate and not because of muscle loss.
I doubt you could gain muscle with this much of a calorie deficit, but subjectively I feel just as strong as I was a month ago.
Heartburn
The most immediate side effect was heartburn, bad enough that I started taking omeprazole. It was a daily occurrence for about a week, and then became something that only seems to happen when I exercise really hard, eat late, or drink alcohol. I try to eat my last meal of the day around 5 pm so I have plenty of time to digest before bed, but 30 days in I can eat at normal times if I have to.
If I did this again, I would take omeprazole for the first week, then the morning after each injection for the second week.
Note: You should not take omeprazole longer than 14 days since your body adapts to it.
Heart Rate
The most concerning side effect was my resting heart rate jumping up and my heart rate variability dropping. I found it significantly more uncomfortable to do cardio like running or hiking (although I found it easier to motivate myself to do moderate workouts).
If I did this again, I'd try tirzepatide, which seems to have less of an effect on heart rate.
Skin Sensitivity
For the first few weeks I'd experience a "tickling", sort-of electric feeling from my clothes.
It was weird and occasionally distracting, but not really a problem, and went away by the end of the month.
Chills
I'm not sure if this was caused by the drug, or the rapid weight loss, but I've turned into a person who freezes in slightly cold rooms. I wear much warmer pajamas, use more blankets, and don't wear shorts as often.
Unfortunately, I didn't measure this before starting, but my core temperature is actually slightly high, hovering around 99° F.
Injection Site Redness
Stabbing a needle into your body makes it upset[citation needed], so I usually get some redness and swelling the day after an injection.
For some reason I didn't get this for the first two weeks, but have had it consistently since. My symptoms are consistent with physical trauma and not infection, so it's annoying but not concerning. Being more careful and steadier with the needle seems to have helped.
Splitting Doses
I had a suspicion that the wild swings in drug concentration over the course of a week were making the symptoms worse, so I switched to 1 mg twice per week for the same total amount but more consistent levels. This subjectively seems to help, although it's annoying that twice the injections means twice the redness and swelling.
Other Effects
Some people think drugs like retatrutide have an effect on motivation, but I disagree. It's just a coincidence that...
..I wrote 1/3rd of the LessWrong posts I've ever written in the last month..
This list actually undersells my writing this month, since I also wrote two additional articles that I decided not to post.
..and started exercising slightly more consistently..
I exercised 17 days in April and May and 13 days in June and July.
..and finally finished that annoying project I was putting off at work..
..and even caught up on my TODO list.
It's weird because I actually do have a good reason for why I suddenly did each of these things: I was inspired by LessOnline and Inkhaven, it was nice out, and the midsummer planning/burnout season was over.
But it does seem kind of suspicious.
A Theory
If retatrutide did help, my guess is that the mechanism is removing distractions. Like I mentioned above, sometimes I'd be working on a post and notice I was getting hungry, then proceed to ignore it and continue writing for a few more hours.
I also find it easier to plan exercise. I don't like to exercise when I'm hungry, but I also don't like to exercise after a heavy meal. Conveniently, I'm never very hungry now, and haven't eaten a heavy meal in over a month.
Maybe the real akrasia was the hunger we had along the way?
Final Thoughts
So, do I recommend injecting yourself with experimental chemicals?
Absolutely not!Losing weight in this way is immoral without the oversight of an IRB, and no IRB would allow such an obvious conflict of interest, where the subject gains significant health improvements in exchange for participating. Also, on a more serious note, retatrutide raising your heart rate is annoying and mildly concerning.
But, maybe do talk to your doctor about an FDA-approved drug like tirzepatide if your weight is causing problems for you. This was way easier than any normal diet, worked better, and the side effects are all manageable, especially if you're prepared.









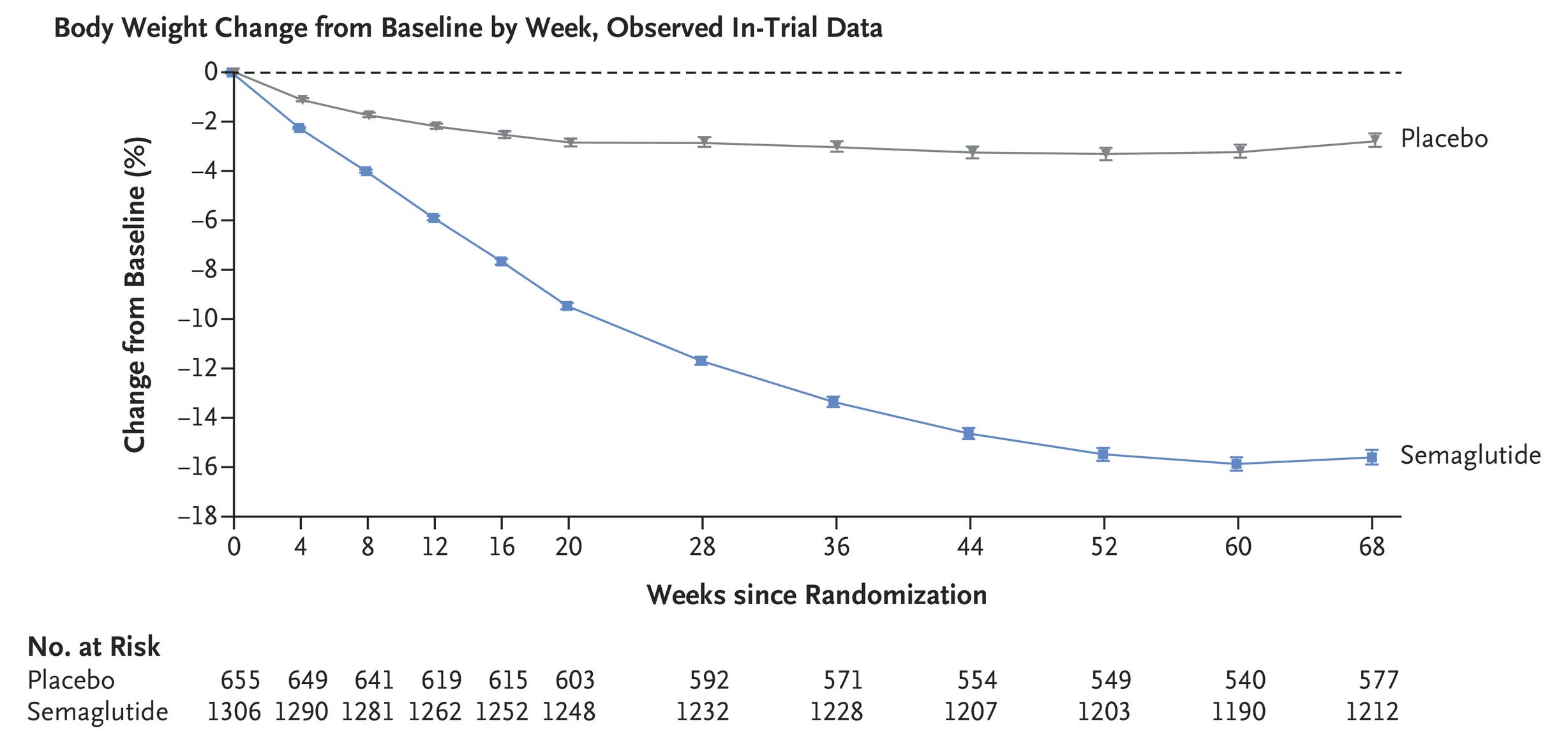
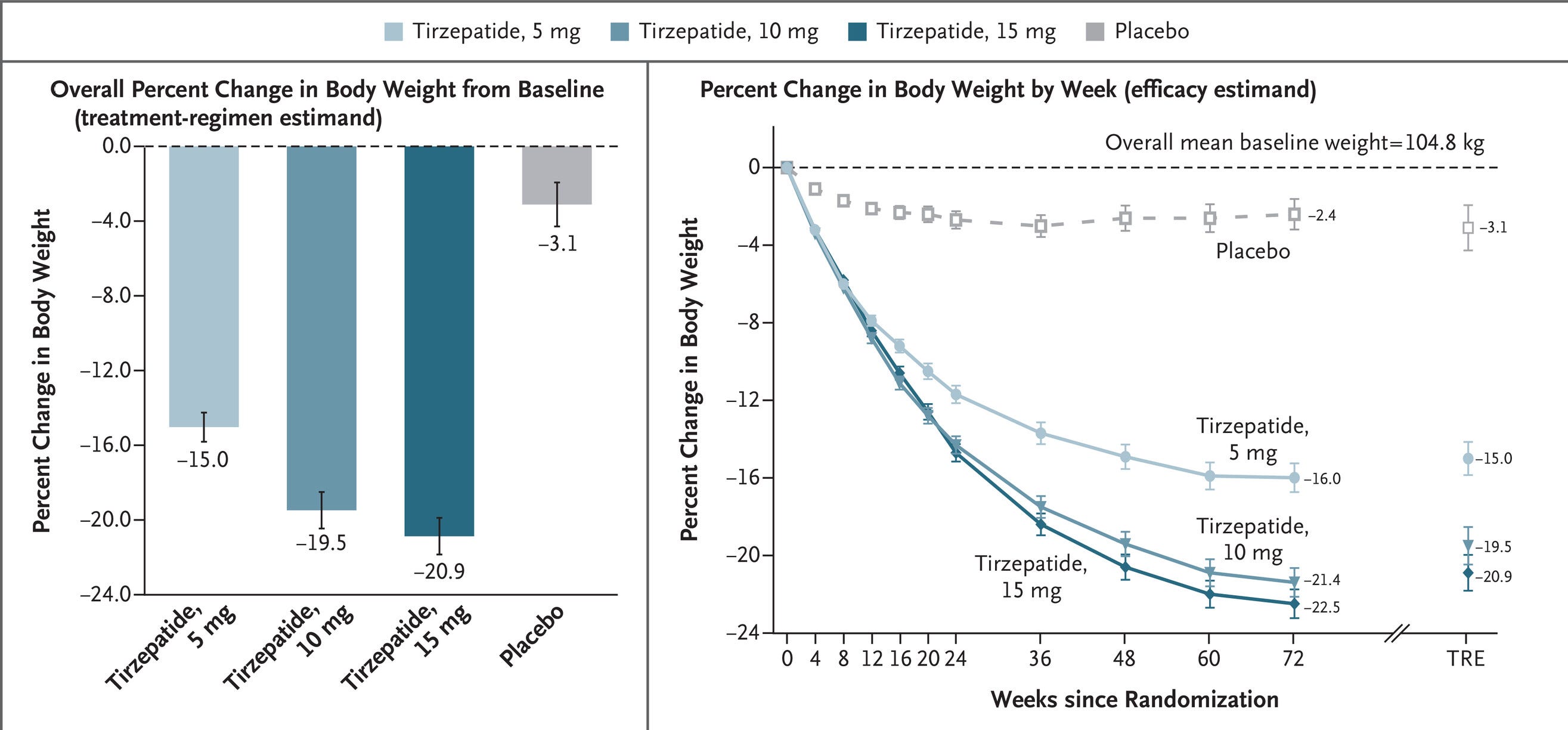
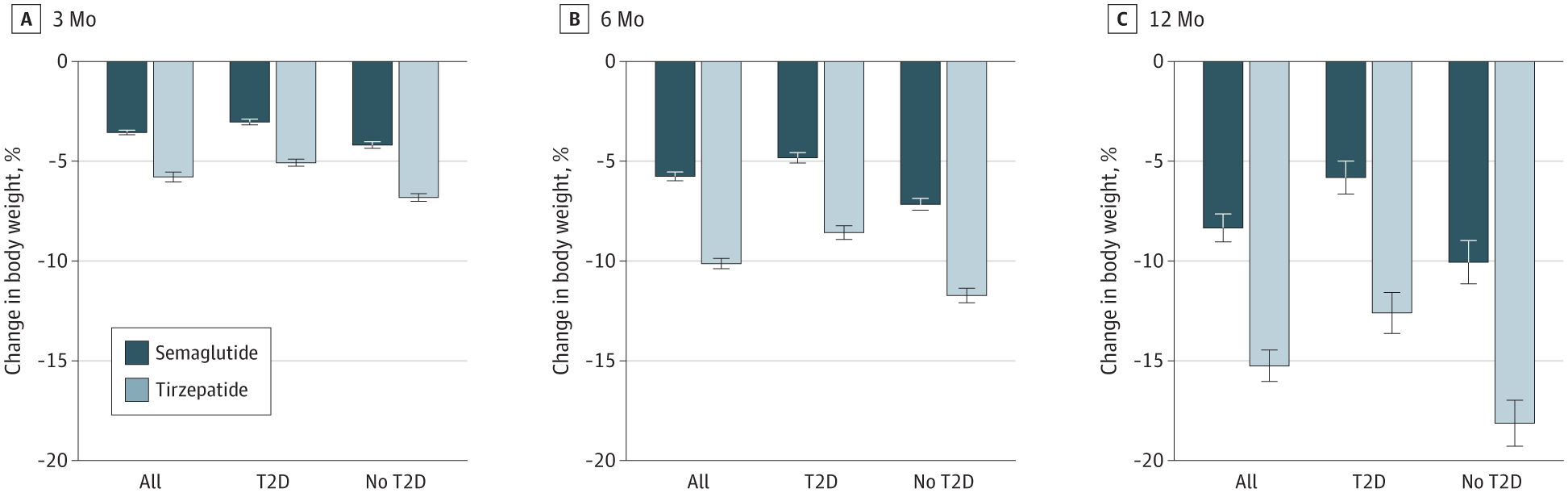
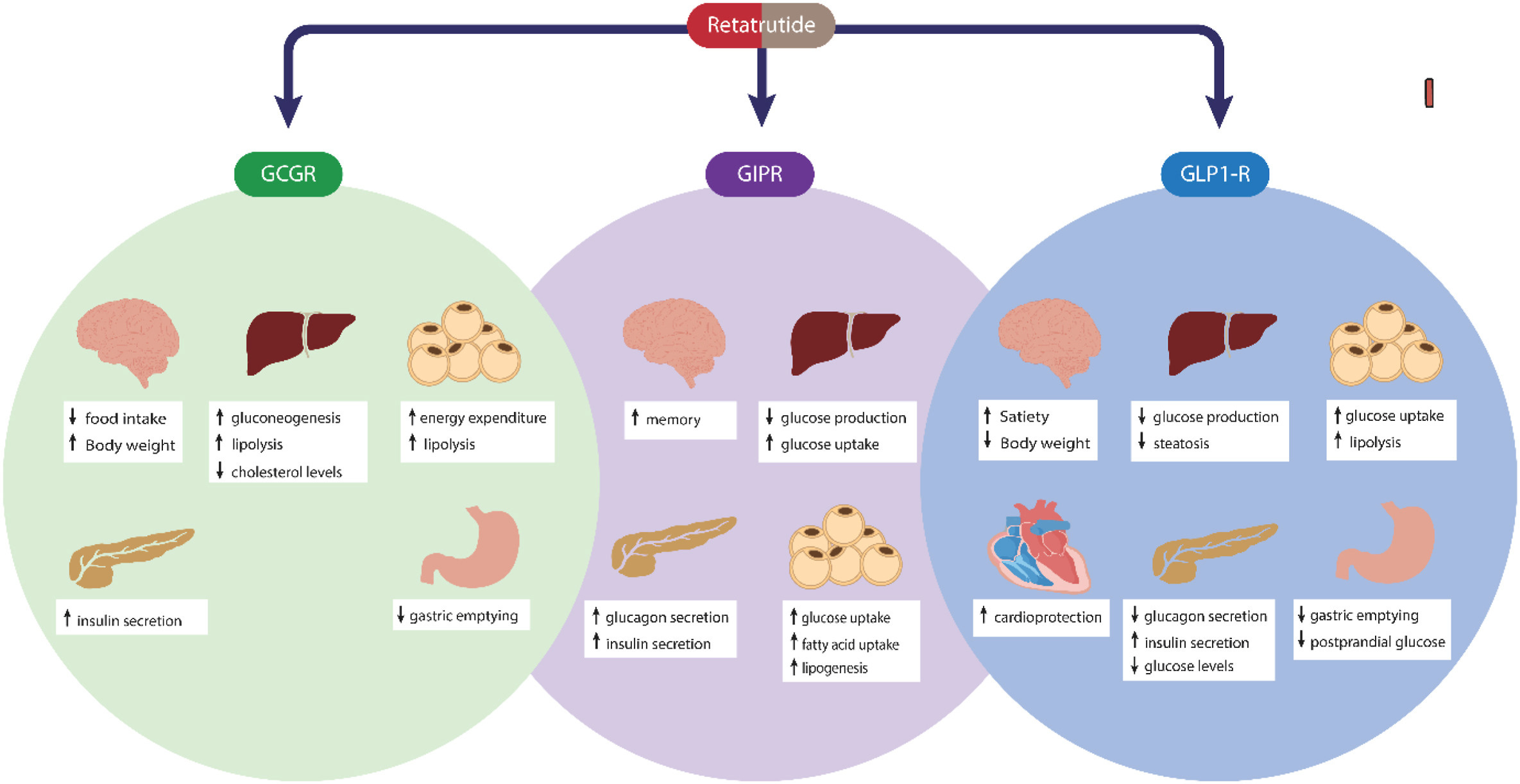


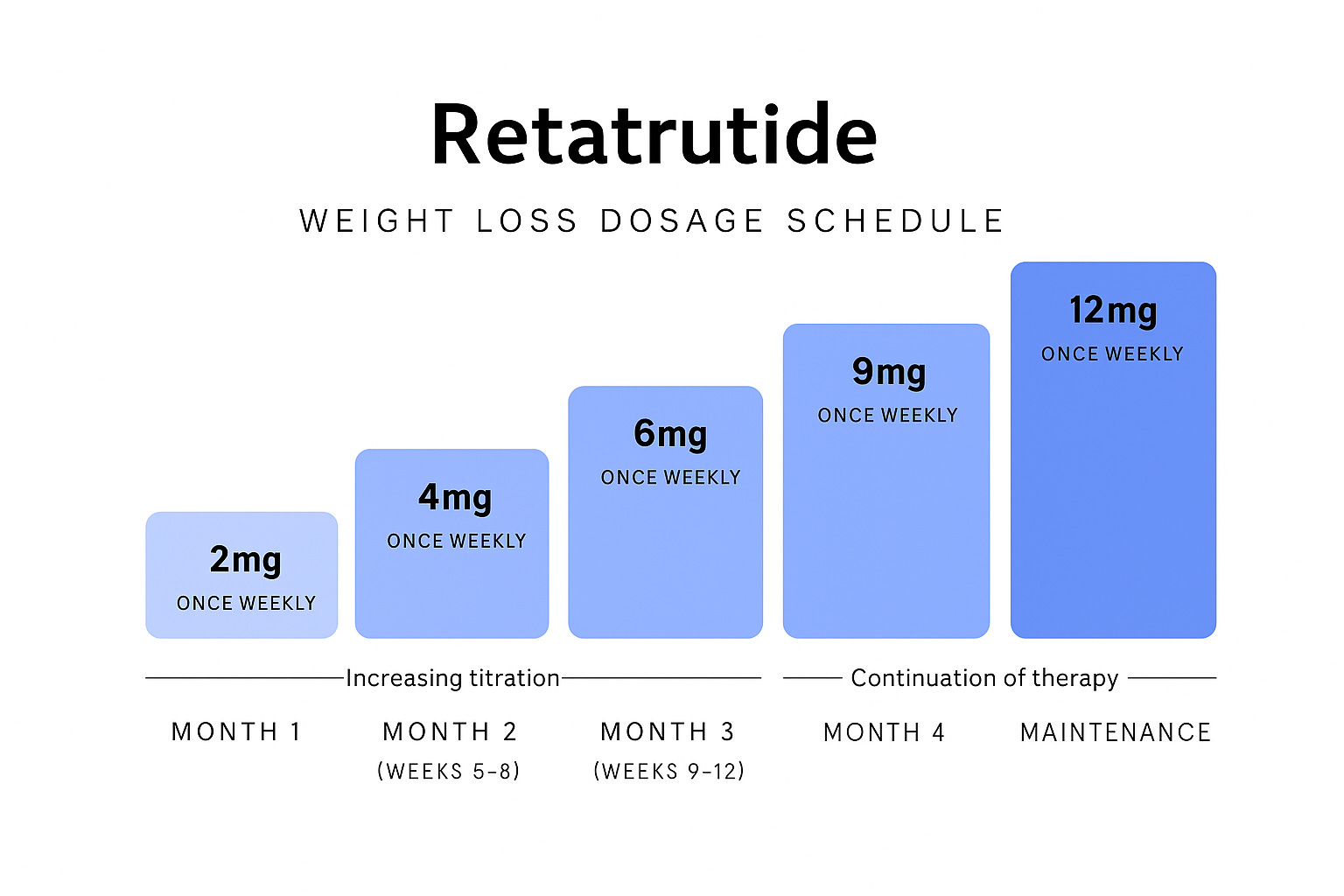








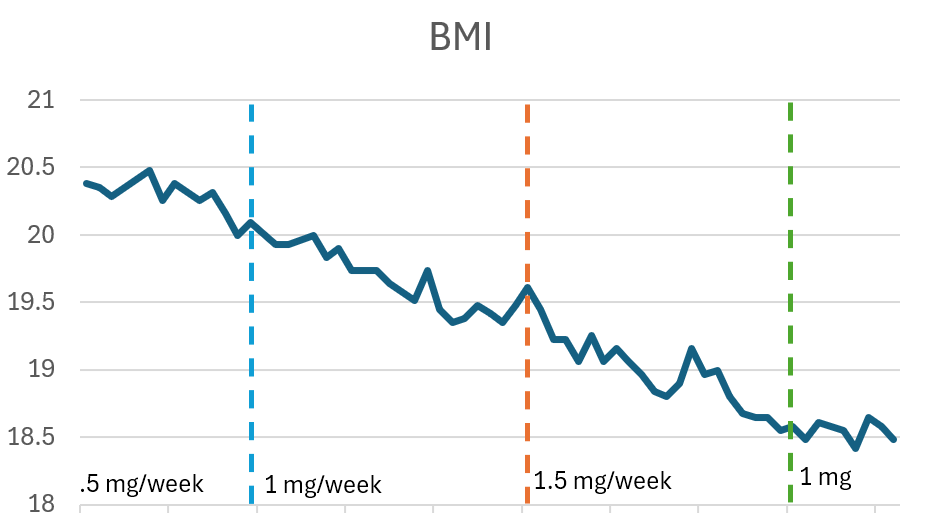
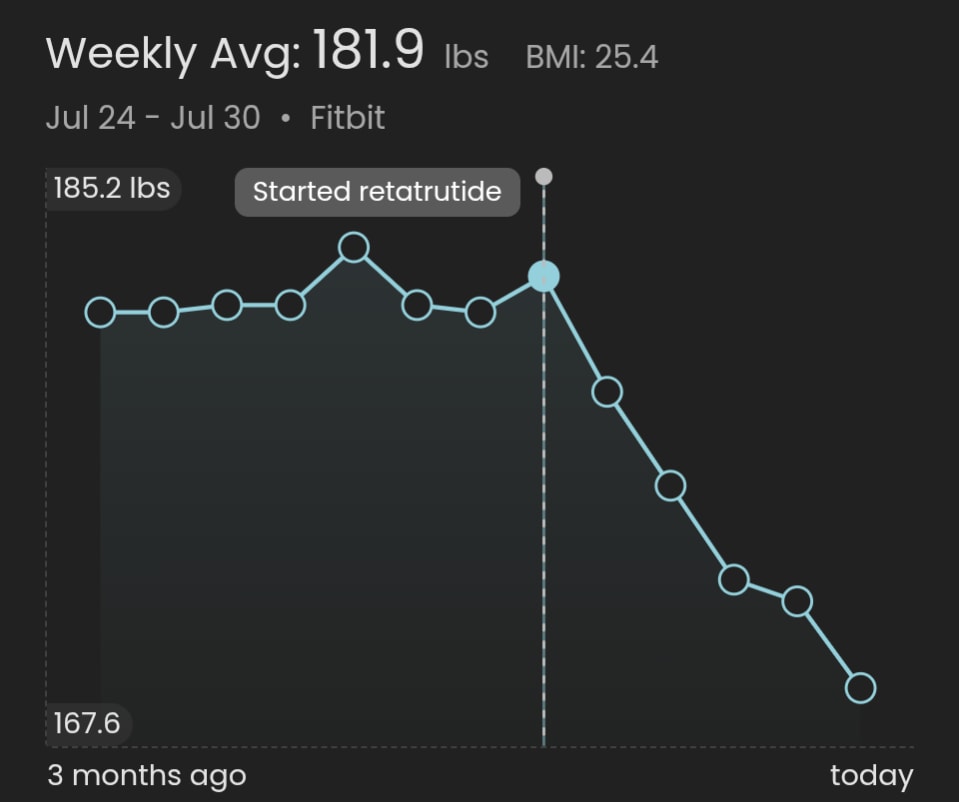
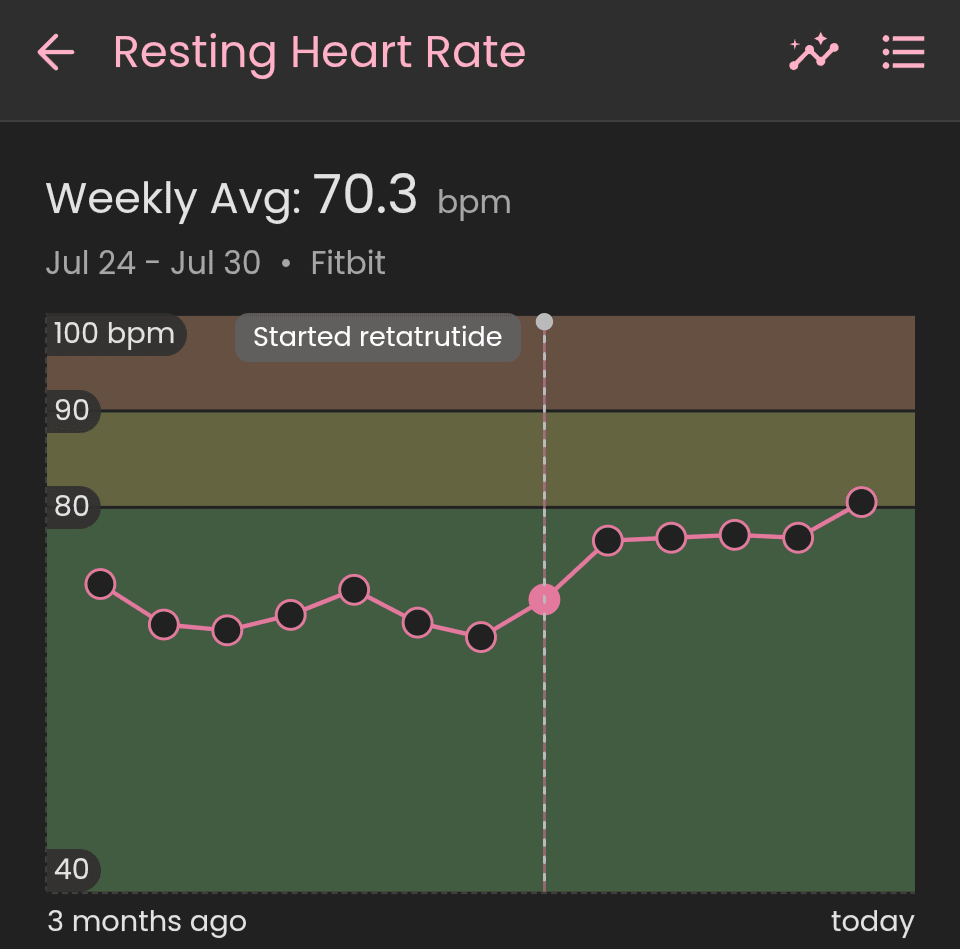
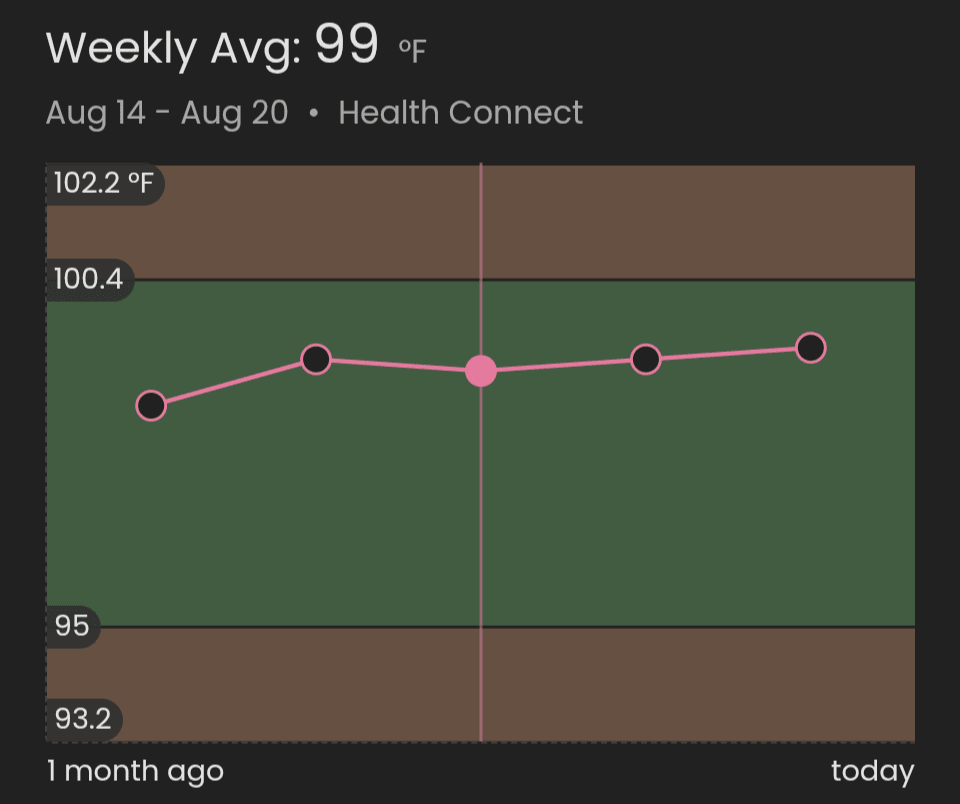
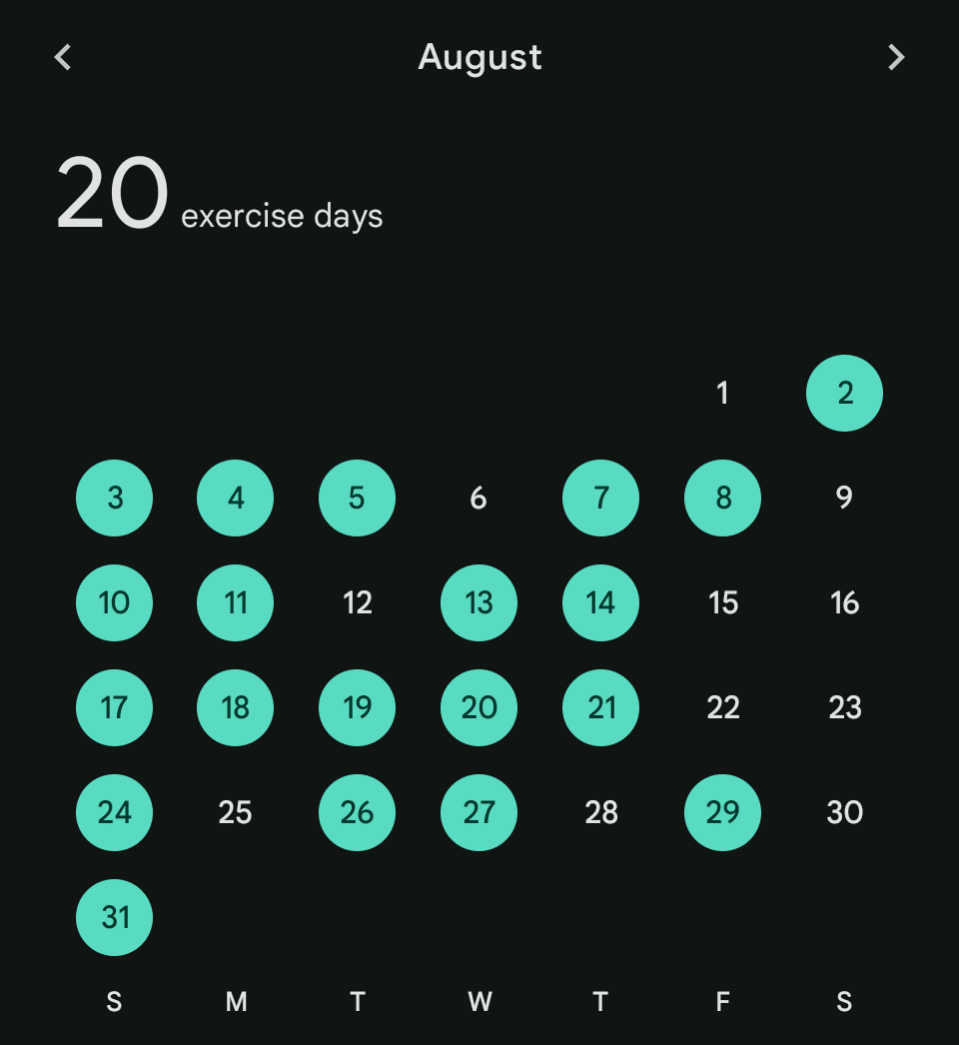

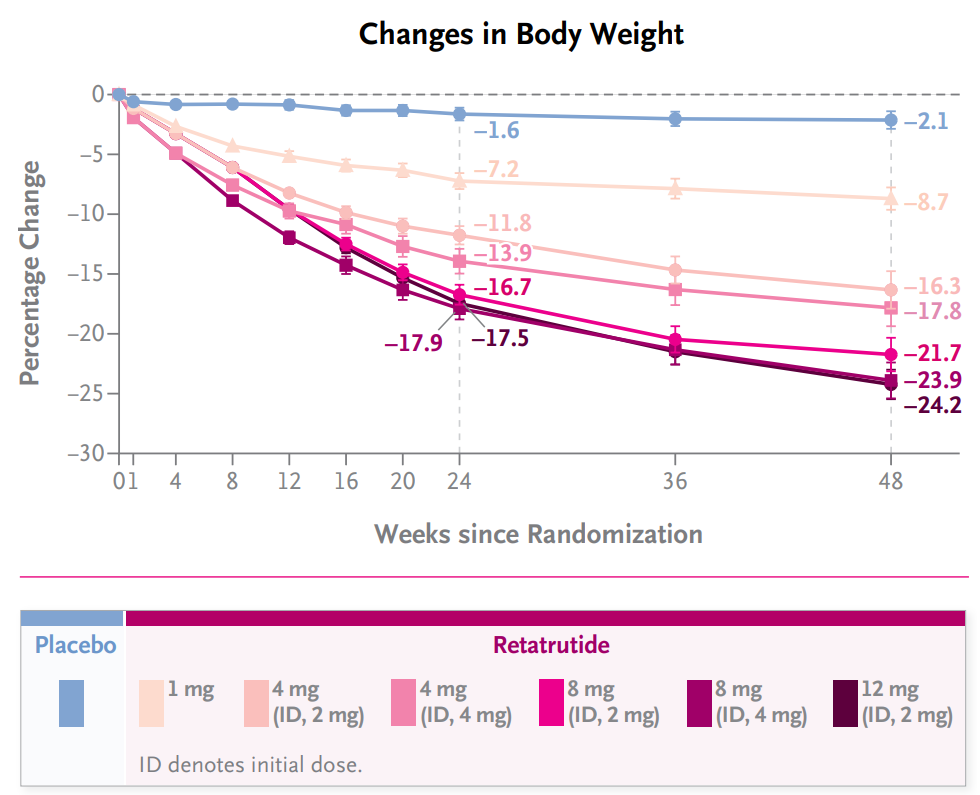{kind=link}
> Diane Yap: I know this guy, SWE manager at a big tech company, Princeton grad. Recently broke up with a long term gf. His idea on how to get back in the dating market? Go to the gym and build more muscles. Sigh. I gave him a pep talk and convinced him that the girls for which that would make a difference aren't worth his time anyway.
Reminder that if you are a man, never take dating advice from a woman.
Regarding the vegetables thing, I do blame Anglos' retarded food culture for the fact that you + Aella etc. don't like veg. In countries with a healthy food culture, vegetables are just an integral part of nice food - curries, spicy hot pots, tasty soups etc. In Anglo food culture, it's mostly if you want a "healthy option", more commonly eaten as salads or joyless boiled green things on the side.
So I think you're missing out if you can't appreciate veg. Even if you think there's something superficially unpleasant about eating veg, to misquote Zvi from two weeks ago, "the failure to experience the sublime in things that people traditionally think are not [delicious] is a Skill Issue",
But, as a big veg lover myself, I'm not actually sure whether it's healthier or not to eat loads of veg. I like liking vegetables, because I like eating (both the social and hedonic aspect), and veg bulks up a meal and extends eating time by 2x or 3x. This probably means I eat slightly less healthily for some meals, because add more fatty/salty sauce to cover the veg appropriately etc. But I'm reasonably effortlessly slim and fit, so take as you will.