diff --git a/docs/index.md b/docs/index.md
index b42cd63..7179a3b 100644
--- a/docs/index.md
+++ b/docs/index.md
@@ -96,14 +96,64 @@ However, there is not that much discussion of this online. Here is all I could f
Regulatory note: Aminophylline is an FDA-listed prescription drug, so supplies intended for human or animal treatment normally require a prescriber’s order or a pharmacy/DEA license; research-grade material from chemical suppliers is labeled *not for human or veterinary use* and should be handled in accordance with local hazardous-chemical regulations. [link](https://www.boundtree.com/pharmaceuticals/rx-pharmaceuticals/aminophylline-25mg-ml-20ml-vial/p/5922-01)
+#### Glycyrrhetinic acid
-#### Transdermal Caffeine
+Much less discussed than aminophylline.
+
+There is like one study from 2005 which seems to suggest a small reduction in a month without negligible weight loss, and it seems like nobody has tried to replicate it:
+
+- [Paper on 9 treatment + 9 control patients](https://pubmed.ncbi.nlm.nih.gov/15894038/){.source-link}
+
+> Weight (kg), before -> after
+>
+> * treated: 60.5 ± 0.6 -> 60.2 ± 0.6 kg
+> * placebo: 59.2 ± 0.4 -> 59.0 ± 0.4 kg
+>
+> Circumference at middle of thigh (cm), before --> after:
+>
+> * treated thigh: 52.7 ± 1.0 --> 52.4 ± 1.0
+> * untreated thigh: 52.9 ± 1.4 --> 52.8 ± 1.4
+> * placebo thigh: 51.9 ± 1.0 --> 51.8 ± 1.0
+> * untreated thigh: 51.1 ± 0.9 --> 51.2 ± 0.9
+>
+> TLDR: 0.3cm difference after 1 month of applying 80mg 2.5% GA daily. minimal change in weight (~0.3kg)
+
+Other studies seem mostly to be in vitro, eg:
+- [in vitro lipolysis study](https://www.sciencedirect.com/science/article/abs/pii/S0006291X12005384){.source-link}
+
+There is even less discussion of GA online/on reddit:
+- [Reddit post from u/Lopsided_Bar2863 on r/4tran4 on aminophylline and glycyrrhetinic acid](https://old.reddit.com/r/4tran4/comments/1eq12mv/poons_theres_a_lifesaver_to_reduce_your_ass/){.source-link}
+
+#### Topical Caffeine
+
+Caffeine appears to affect the same PDE pathway as aminophylline, but there are not many studies using just caffeine.
+
+Some examples:
+
+* [study on 7% caffeine for cellulite](https://pubmed.ncbi.nlm.nih.gov/17524126/){.source-link}
+> "They were told to apply it in just one leg (thigh and hip) in order to keep the other one as control. The solution was applied twice daily (morning and night), and the dose was ∼15 mL per leg (thigh)."
+>
+> "99 completed the protocol"
+>
+> "A 30-day treatment with this caffeine solution showed statistical significance concerning the reduction of circumference in treated thighs. This reduction was observed in more than 80% of the patients and was of about 2.1 cm in the thicker portion of the thigh and 1.7 cm in the lower portion. The use of 7% caffeine solution was also statistically significant in the reduction of hip circumference in 67.7% of the treated patients."
+
+* [study on 3.5% caffeine for cellulite](https://pubmed.ncbi.nlm.nih.gov/26082579/){.source-link}
+> Thigh and upper-arm circumferences decreased by 0.7 cm (1.7%) and 0.8 cm (2.3%), respectively, at week 6. (No control was provided).
+
+
+* [Study on caffeine + retinol + carnitine + others](https://pmc.ncbi.nlm.nih.gov/articles/PMC3933246/){.source-link}
+> Maintain usual diet + twice daily (caffeine + retinol + carnitine + others).
+> 12 weeks treatment:
+>
+> Abdomen: −1.1cm (vs −0.4cm)
+> Thighs: -0.8cm (vs −0.3cm)
+> Hips: −0.8cm (vs −0.4cm)
Transdermal caffein
#### Waist-training
-As another option, if looking particularly to improve WHR or get a more hour-glass figure, could be waist training. This can often reduce appetite while worn. If done correctly this is usually quite safe, thought this does often cause the floating ribs 8-12 to shift inwards, and may cause some organs to move around.
+As another option, if looking particularly to improve WHR or get a more hour-glass figure, could be waist training. This can often reduce appetite while worn. This usually is done by causing the floating ribs 8-12 to shift inwards, and may cause some organs to move around. People who do it consider it safe but DYOR.
#### Rib reshaping surgery
diff --git a/docs/sources/old-reddit-com__r-4tran4-comments-1mlcyaf-what_cis_girls_get_done_vs_what_tr__9285331de2.html b/docs/sources/old-reddit-com__r-4tran4-comments-1mlcyaf-what_cis_girls_get_done_vs_what_tr__9285331de2.html
new file mode 100644
index 0000000..4ec1221
--- /dev/null
+++ b/docs/sources/old-reddit-com__r-4tran4-comments-1mlcyaf-what_cis_girls_get_done_vs_what_tr__9285331de2.html
@@ -0,0 +1,375 @@
+
+
+
+
+
+
What cis girls get done VS what trans girls get done
+
r/4tran4 • by u/TheForceOfEvil • 42 points
+
Making your shoulder fat slouchy and destroying your collarbones for WHAT?!
+
Is it in proportion with your waist, hips and ribcage now?! Cuz if you already have a wide ribcage this will only make it look worse especially if you have a masc ribcage and fem shoulders it will throw off the balance.
+
I think you can tell when a girl(cis or trans) Centers men and sees things from the male gaze instead of female gaze depending on the surgeries she gets
+
Ex. Boob job + BBL VS Rhinoplasty + Brow lift
+
+
+
Comments
+
+
+
+ u/jellybeanzz11 • 15 points
+
+
+
the difference is ropefuel...
+
+
+
+
+
+ u/TheForceOfEvil • 18 points
+
+
+
It literally looks like she gained 50 pounds it doesn’t even look smaller and it’s so expensive too. Any girl would kill to have these collarbones wtfff
+
+
+
+
+
+
+
+ u/WanderingWonders77 • 13 points
+
+
+
I'm not really impressed with clavicle reduction tbh. the slouch doesn't seem worth it (it looks even worse from the side tbh)
+
t. bideltoidhon
+
+
+
+
+
+
+ u/F2Misanthrope • 7 points
+
+
+
would it be possible to get clavical shortening and then the shoulder unslopening
+
+
+
+
+
+
+ u/You-Looked • 8 points
+
+
+
This shit is hopeless
+
+
+
+
+
+
+ u/Impressive_Fish3957 • 3 points
+
+
+
trap botox only lasts a few months while surgery is permanent so this isn't a fair comparison. i do agree with you that the first photo looks better though
+
+
+
+
+
+
+ u/zunCannibal • 4 points
+
+
+
collarbones on 2nd pic looked like they were about to escape
+
+
+
+
+
+
+ u/blown-transmission • 4 points
+
+
+
Ugly passoid or slightly clocky elf woman
+
Choice is yours
+
+
+
+
+
+ u/New-Tie-2255 • 1 points
+
+
+
ugly passoid
+
+
+
+
+
+
+
+ u/notdyingb4ffs • 4 points
+
+
+
clavicle reduction seems like a surgery for stupid or rich ppl atp. like you said it’s cope because what actually matters is how your WHR and ribcage flow into your shoulders. your body needs to look balanced and it’ll look disproportionate like a girl that never works out getting a BBL.
+
trans women are better off getting a BA to offset their larger ribcages while getting better posture. i see so many tgirls complaining about their upper bodies while having awful posture, slouching makes you look a lot wider and looks worse!
+
+
+
+
+
+
+ u/Delicious-Raise-17 • 3 points
+
+
+
Trans women are nothing like cis women, unfortunatly
+
+
+
+
+
+
+ u/wistfulfaerie • 2 points
+
+
+
It’s over 😞
+
+
+
+
+
+
+ u/summer-years • 3 points
+
+
+
Genuinely ty for reminding me that this cope I've been dreaming about is regarded and that I need to corsetmaxx or smthn
+
+
+
+
+
+
+ u/Jamtlanta • 1 points
+
+
+
If more horizontal shoulders still look feminine, what makes them look masculine? Is it just the breadth? I'm a pooner with sloped shoulders and can't tell if they look better or worse when I try to shrug them up because doing that decreases the shoulder breadth and neck length.
+
+
+
+
+
+
+ u/Intelligent-Tea-2058 • 1 points
+
+
+
+
Is it in proportion with your waist, hips and ribcage now?! Cuz if you already have a wide ribcage this will only make it look worse especially if you have a masc ribcage and fem shoulders it will throw off the balance.
+
+
I plan to go for complete center surgery for this reason (insurance pending, inb4 denial fight)
+
I will lyk if it works for the dysphoria and if I'm more uggo after or not
+
+
+
+
+
+ u/atillathetwink • 2 points
+
+
+
I don't think I've heard of complete center surgery before, is it something that actually reduces your whole ribcage? I really need something like that but ive only seen it referenced once there's not a lot of information I can find about whether its even possible
+
+
+
+
+
+ u/Intelligent-Tea-2058 • 4 points
+
+
+
It's a joke, given how people talk about top and bottom surgery... (I cringe at these new terms thh) why not "center surgery"?? 🥺 my thorax needs fixing 🥺
+
What I am seeking though is:
+
+
Scapula Reduction
+
Clavicle Shortening
+
Thoracic Feminization/Reduction / Full Ribcage Resection (no clear name yet for it, getting tried on a cadaver soon last I checked) - TL;DR: remove strip of cartilage either side of sternum and secure with absorbable plates and screws
+
Lower rib resection w/ costal flare reduction
+
Floating rib fracture and reset or removal
+
Pelvic plasty, possibly (Ti illiac augmentation + silicone hip implants)
+
Maybe a modified form of triple pelvic osteotomy and other pelvic reconstruction, if it can be developed for us
+
+
Surgery worked everywere else HRT couldn't so far, why not try it here? If I pull this off maybe I can be 99% cured, and these techniques can be spread if developed. I am nuts enough to go first if I can fund it, and have been doing insanely dangerous work with that goal, sustaining multiple injuries along the way. I am dysphoric AF and will do almost anything to get free. People say I'm just "wormed" badly... they have no fucking idea. I was "wormed" enough to troon out as a kid in the 00s... of course I'm going to fight till no worm remains. Once made whole through the power of bright lights, cold steel, and another day or two of propofol pseudo brain death, my powers will no longer be dissapated by physical dysphoria. I hope I can help lots of tranners get better thereafter. If any of my body can be recovered after whatever brings about my untimely demise someday, I hope I can be studied in a pro-trans lab to enhance future trannies.
+
+
+
+
+
+ u/atillathetwink • 2 points
+
+
+
Yeah that "thoracic feminization" is what I'm interested in. I've never heard anything about it except for one other person on here mentioning it. Do you have any other sources of information about it you could share with me? The fact that it needs to be tested on a cadaver implies its still very theoretical which sucks, I was under the impression that it was close enough to surgeries that are already performed on cis people that it was decently well understood already. Also, is there reason to believe it would even do much? It seems like there can't possibly be enough cartilage to remove to actually make a big enough difference in size. I guess it's probably pretty unrealistic for me to expect it to fix me but I'm still really curious if you have any more info. And huge respect for your surgerymaxxing plan btw I wish you the best of luck.
+
+
+
+
+
+ u/Intelligent-Tea-2058 • 1 points
+
+
+
Basically a U.S. surgeon with some others, a Chinese thoracic surgeon, and maybe one other team are each working towards it in some way. I am concerned some of the EOs and intimidation will limit how much one once-interested medical system will provide.
+
+
It seems like there can't possibly be enough cartilage to remove to actually make a big enough difference in size.
+
+
Apparently 1 inch of circumference per side seems possible, perhaps more especially paired with other things.
+
I'll DM you.
+
+
+
+
+
+
+
+
+
+
+ u/atillathetwink • 1 points
+
+
+
so wait, are you for or against clavicle shortening? you imply you don't think it looks good but also imply its good because it doesn't center the male gaze?
+
+
+
+
+
+
+ u/Important_Ad_7416 • 1 points
+
+
+
what if I have a small ribcage?
+
Ive seen a girl who went from inverted triangle to hourglass with clavique alone
+
+
+
+
+
+ u/TheForceOfEvil • 1 points
+
+
+
What are your measurements? Regardless of your size I hope your surgeon does a good job so you don’t end up with slouchy undefined shoulders and no collarbones, because that’s worse than having 2 extra inches imo.
tbhon i couldnt care less about how undefined my shoulders are so long as they're small
+
+
+
+
+
+ u/TheForceOfEvil • 2 points
+
+
+
I Actually have similar measurement! 70cm with 40cm. Honestly it depends on your height and weight? I think gaining a bit of weight for me to round up hips could be enough plus I am 174cm so I think it can be proportional.
+
ALSO remember wide shoulders are needed to have an hourglass body shape unless you’re going for a pear shaped body, regardless of your goals if you can afford it(aka Starbucks or amazon insurance) and truly want it go get it but make sure they do a good job cuz some of the results I’ve been seeing have been looking awful.
+
I just don’t want girls to be basically hunting a stereotypical look of femininity. Just because society tells you you need to be small and submissive to be a worthy woman that doesn’t mean you have to actually do it ❤️❤️❤️
+
+
+
+
+
+ u/Important_Ad_7416 • 1 points
+
+
+
mogged 😓
+
im too broke for it and living in europe, im just gonna put on weight snd hope for the best
+
+
+
+
+
+
+
+
+
+
+ u/46XX_ • 1 points
+
+
+
Broad shoulders are literally pretty? bulky ones just aren't bc they add alot of visual mass😭
+
+
+
+
+
+ u/Important_Ad_7416 • 3 points
+
+
+
that's gonna be my cope
+
haha so pretty, so stunning, i love being build like a coathanger just like a man i mean model, i love looking like that and dont seethe when i see girls with tiny shoulders that match their hips
+
+
+
+
+
+ u/46XX_ • 0 points
+
+
+
Having broad but "lean" shoulders isn't being build like a man, that what most models have😭
+
Them being bulky n broad is manly.
+
+
+
+
+
+ u/Important_Ad_7416 • 1 points
+
+
+
Ok but I'm 163cm I'm never pulling off the model look and also dont like it 😓
An integral topical gel for cellulite reduction: results from a double-blind, randomized, placebo-controlled evaluation of efficacy
+
Abstract
+
Background
+
Cellulite is a serious cosmetic concern for most of the 90% of women affected by it.
Objective
+
To assess the clinical efficacy of a complex integral anti-cellulite gel.
Methods
+
This double-blind, randomized, placebo-controlled study involved 44 healthy women, aged 25–55 years. Subjects had a normal to slightly overweight body mass index and presented slight to moderate cellulite on their thighs, buttocks, and/or hips at baseline. Subjects were randomly assigned to either the treated or placebo group and accordingly applied the active product or placebo on their hips, stomach, buttocks, and thighs, twice daily for 3 months. Skin tonicity, orange-peel aspect, and stubborn cellulite were assessed at day 0, 28, 56, and 84. A self-evaluation questionnaire was completed by all volunteers.
Results
+
At the end of the study, an average of 81% of the subjects applying the active product presented improvement in their cellulite condition versus 32% for the placebo group (all descriptors and sites combined). At day 84, skin tonicity, orange-peel appearance, and stubborn cellulite were improved in a significant manner (P<0.05) over placebo, on all studied areas. Skin tonicity improved on average by +41% for buttocks, +35% for hips, and +31% for thighs. Orange peel appearance was reduced on average by −25% for buttocks, −22% for hips, and −22% for thighs. Stubborn cellulite was reduced on average by −19% for buttocks, −24% for hips, and −22% for thighs. Circumference measurements decreased in a significant manner (P<0.05) over placebo, for the abdomen (average value of −1.1 cm) and thighs (average value of −0.8 cm). The product was well tolerated and perceived by the volunteers themselves as better performing than placebo on all criteria.
Conclusion
+
All results validate the efficacy of the present integral formulation to significantly reduce signs of cellulite and reshape the silhouette.
Cellulite refers to a local alteration of the relief of the skin which acquires an orange-peel, or mattress, appearance. The orange-peel appearance results from the bulging of fat lobules out of their connective frame, into the dermis. The phenomenon is most commonly seen on hips, buttocks, and thighs but can also touch other areas, including the abdomen. Up to 90% of woman, over 20 years of age, are affected at various degrees, against only 2% of men.1–3 Cellulite is seen as a normal condition by the medical community, but it is a serious cosmetic concern for most women affected by it.
+
Although cellulite involves fat cells, it is not a manifestation of obesity, and even young women with a normal body mass index (BMI) may get it.4 However, being overweight aggravates the presence of cellulite. Other risk factors include a predisposing genetic background, hormonal imbalance, medication that causes water retention, a sedentary lifestyle, prolonged periods of immobility, wearing tight clothes, smoking, excessive alcohol intake, unhealthy eating habits, stress, and being Caucasian.5 Some disorders have also been associated with cellulite, such as venous insufficiency, kidney problems, metabolic perturbations, and gastrointestinal alterations.5
+
The exact etiology of cellulite is still a matter of debate, but most scientists will agree on the involvement of reduced microcirculation, interstitial liquid infiltration (edema), localized hypertrophy of adipocytes, oxidative stress, and persistent low grade inflammation, combined with extracellular matrix alterations.4,6–9 The extensibility, elasticity, and resilience of the skin are also abnormal.10
+Figure 1 schematizes all these elements. The condition may start with hormone-induced activation of matrix-metalloproteinases (MMPs), which weakens capillary walls and challenges extracellular matrix integrity.11 As a result, fluid leaks out of vessels, and inflammatory cells are recruited within tissues where they generate inflammation and release additional MMPs. In an effort to heal, the damaged matrix of the septa becomes fibrosclerotic.7 Meanwhile, hormones may also stimulate the metabolic activity of adipocytes, which increase in volume. Hypertrophic fat lobules tend to exert pressure on the surrounding capillaries, therefore adding to their fragility and hampering circulation.10
+
Figure 1.
+
+
Major mechanisms involved in cellulite. The exact etiology of cellulite is still a matter of debate but most scientists agree on the involvement of reduced microcirculation, interstitial liquid infiltration (edema), localized hypertrophy of adipocytes, oxidative stress, and persistent low grade inflammation, combined with ECM alterations. Cellulite and skin aging may influence each other.
+
Abbreviation: ECM, extracellular matrix.
The process is a reminder of what happens with aging in the upper layers of skin (dermis and epidermis) where changes are associated with MMP activation, altered biomechanical properties, reduced vessel integrity, and inflammation. Indeed, a clinical study conducted by Ortonne et al12 confirmed that the presence of cellulite precipitates skin aging in women over 30 years of age. Therefore, it may be advisable to address both conditions simultaneously when treating cellulite. The approach described in this paper follows this lead. The test product is an integral gel, simultaneously addressing skin aging and cellulite. The patent-pending13 formula combines all active cosmetic ingredients listed in Table 1. The final concentration of cosmetic active ingredients in the formulation reaches 25% (weight per weight [w/w]).
+
Table 1.
+
Actives versus proposed actions on skin. List of all active ingredients found in IDC™ (Immanence IDC Inc, Québec, QC, Canada) anti-cellulite gel, with their proposed actions on skin, according to published literature and/or patent documents
+
+
+
+
Actives versus proposed actions (with reference number)
+
+
Anti-aging
+
+
+
+
+
Anti-cellulite
+
+
+
+
+
+
↓Adipogenesis
+
↓Lipogenesis
+
↑Lypolysis
+
↑Microcirculation
+
↑ECM synthesis
+
↑ECM integrity
+
↓Inflammation
+
↓Oxidation
+
↑Hydration
+
↑Barrier
+
↑DNA protection
+
↑Energy
+
↑Oxygenation
+
↑Immunity
+
↓Pigmentation
+
Keratinization
+
↑Skin cohesion
+
↑Cell anchorage
+
↓Glycation
+
+
+
+
+
Adenosine
+
+
+
+
+
29
+
30
+
29
+
+
+
+
+
31
+
32
+
+
33, 34, 35
+
34, 36
+
+
37
+
+
+
+
+Alteromonas ferment extract
+
+
+
+
+
+
+
+
+
+
38
+
+
+
+
38
+
+
+
+
+
+
+
+
Ascorbic acid
+
+
+
+
+
39
+
39
+
+
8
+
+
+
+
+
+
+
40
+
+
41
+
42
+
43, 44
+
+
+
a-Bisabolol
+
+
+
+
+
+
+
45, 46
+
46, 47
+
+
46, 48
+
+
+
+
+
46, 49, 50
+
+
+
+
+
+
+
Caffeine
+
+
8, 51
+
8, 18, 51
+
15, 51
+
+
+
+
51, 52
+
+
+
+
+
+
+
+
+
+
+
+
+
+
Caprylic/capric triglyceride
+
+
+
+
+
+
+
+
+
53
+
+
+
+
+
+
+
+
+
+
+
+
+
Carica papaya extract
+
+
+
+
54
+
+
+
54
+
+
+
55
+
+
+
+
+
+
+
+
+
+
+
+
Carnitine
+
+
+
56
+
+
57
+
+
+
58
+
+
59
+
+
58, 60
+
+
+
+
18
+
+
+
+
+
+
Centella asiatica extract
+
+
+
+
54
+
54, 61, 62, 63
+
+
54
+
64
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+Chenopodium quinoa seed extract
+
65
+
+
65
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+Coleus forskohlii extract
+
+
+
18, 66
+
+
+
+
+
+
+
+
67
+
+
+
+
+
+
+
+
+
+
+
Creatine
+
+
+
+
+
68
+
+
+
69
+
+
+
70
+
71
+
+
+
+
+
+
+
+
+
+
Dipalmitoyl hydroxyproline
+
+
+
+
+
72
+
73, 74
+
+
+
72, 75
+
72, 75
+
+
+
+
+
+
72
+
+
74
+
+
+
+
Dipeptide-2
+
+
+
+
76
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
Escin
+
+
+
+
77, 78, 79
+
+
77
+
77, 79
+
78
+
+
+
+
+
+
+
+
+
+
80
+
+
+
+
Ethylbisiminomethylguaiacol-manganese chloride
+
+
+
+
+
+
+
81
+
82
+
+
+
83
+
+
84
+
+
+
+
+
+
+
+
+
Glutathione
+
+
+
+
+
+
+
+
85
+
+
+
+
85
+
+
+
86
+
+
+
+
+
+
+
Glycerine/glycerol
+
+
+
+
+
+
+
+
+
87, 88
+
87
+
+
+
+
+
+
+
+
+
+
+
+
Glycyrrhizate (licorice extract)
+
89
+
89, 90
+
89
+
+
+
91
+
92, 93, 94
+
91, 92
+
+
94, 95
+
+
+
+
+
96
+
+
+
+
+
+
+
+Hedera helix extract
+
+
+
+
54, 79, 97
+
77
+
+
98
+
99
+
+
+
+
+
+
+
+
+
+
+
+
+
+
Hesperidin methyl chalcone
+
+
+
+
76
+
+
+
100
+
101
+
+
102
+
103
+
+
+
+
104
+
102
+
+
+
105
+
+
+
+Imperata cylindrica extract
+
+
+
+
+
+
+
+
+
106
+
+
+
+
+
+
+
+
+
+
+
+
+
Iris (iris) florentina extract
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
107
+
107
+
+
+
+
+
+
+Kigelia africana extract
+
+
+
+
108
+
108
+
+
109
+
108
+
+
108
+
+
+
+
+
+
108, 110
+
+
+
+
+
+
+Lotus maritimus leaf extract
+
111
+
+
111
+
+
+
+
111
+
111
+
+
+
+
+
+
+
+
+
+
+
+
+
+
Lupine protein
+
+
+
+
112
+
112
+
113
+
112
+
114
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+Medicago sativa seed extract
+
+
+
+
+
115
+
115
+
+
+
+
+
+
+
+
+
+
115
+
+
+
+
+
+
+Nelumbo nucífera leaf extract
+
116, 117
+
+
116, 117
+
+
+
116
+
116
+
118
+
+
+
+
+
+
+
+
+
+
+
+
+
+
Palmitoyl oligopeptide
+
+
+
+
+
119, 120
+
119, 121
+
122
+
122
+
+
+
+
+
+
+
+
123
+
124
+
+
+
+
+
Palmitoyl tetrapeptide-7
+
+
+
+
+
+
+
125
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
Pentapeptide-25
+
117, 126
+
117, 126, 127
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
Polyglucuronic acid
+
128, 129
+
128, 129
+
128, 129
+
+
128, 129
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
Retinol
+
8
+
+
+
130, 131
+
132, 133
+
132
+
133, 134
+
88
+
135
+
+
+
+
+
136
+
137
+
18, 138
+
130, 131
+
+
+
+
+
+Rumex occidentalis extract
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
139, 140
+
+
+
+
+
+
+
+Ruscus aculeatus root extract
+
+
+
+
54
+
+
77
+
141
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
Sesame seed oil
+
+
+
+
+
+
142
+
142
+
143, 144
+
+
+
+
+
+
+
+
145
+
+
+
+
+
+
Sodium hyaluronate
+
+
+
+
+
+
+
146
+
+
147
+
148, 149
+
+
+
+
150
+
+
+
+
151
+
+
+
+
Sodium salicylate
+
+
+
+
+
152
+
+
153
+
+
+
+
154
+
+
+
+
+
155
+
+
+
+
+
+
Squalane
+
+
+
+
+
+
+
+
156, 157
+
156, 157
+
156, 157
+
+
+
+
+
+
+
+
+
+
+
+
TEA-hydroiodide
+
+
+
158, 159
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+Theobroma cacao extract
+
+
8, 160
+
8
+
+
+
161
+
161, 162
+
161, 163
+
+
+
+
+
+
+
+
+
+
+
+
+
+
Tripeptide-1
+
+
+
+
+
164
+
+
164, 165
+
164
+
+
+
+
+
+
+
166
+
167
+
+
167
+
168
+
+
+
Tocopheryl acetate
+
+
+
+
+
+
+
169
+
8, 169
+
170
+
170
+
169
+
+
+
+
169
+
170, 171
+
+
+
172
+
+
+
Ubiquinone
+
+
+
+
+
173
+
174
+
174
+
175
+
+
+
175
+
71, 175, 176
+
175
+
+
+
+
173
+
+
+
+
+
Urea
+
+
+
+
+
+
+
+
+
177
+
177
+
+
+
+
+
+
178
+
+
+
+
+
+
Wheat germ oil
+
+
+
+
+
+
+
+
179
+
180
+
+
+
+
+
+
+
+
+
+
+
+
+
+
The skin anti-aging aspect of the formulation integrates multiple ingredients addressing all major known mechanisms involved in the process. The components, rationale, and efficacy of this anti-aging approach have been described previously elsewhere.14 For their part, the anti-cellulite ingredients were selected on the basis of their potential complementarities in addressing the cellulite problem on all fronts, according to published literature. They include cosmetic ingredients with well documented anti-cellulite activity, such as caffeine, retinol, forskolin (Coleus forskohlii), sacred lotus (Nelumbo nucifera), carnitine, and escin, among others. For a list of all ingredients present in the formulation and their respective expected action on skin, please refer to Table 1.
+
Many of the ingredients included in this formulation have proven their anti-cellulite efficacy in published human clinical studies. For instance, caffeine is a known stimulator of lipolysis, through inhibition of phosphodiesterase and increased adenosine monophosphate levels in adipocytes,2 and has had its slimming activity clinically confirmed by Lupi et al.15 As is the case for the present formulation, caffeine may be vectorized with phospholipids to facilitate skin absorption.16 As was done here, caffeine may also be mixed with other active ingredients for improved performance. Indeed, a mixture of caffeine and N. nucifera extract was shown by Escudier et al to enhance the benefits of a healthy diet for the treatment of cellulite.17 A synergistic mixture including caffeine, carnitine, forskolin, and retinol was also reported by Roure et al18 to improve several parameters linked to cellulite. Moreover, a mixture of retinol, caffeine, and ruscogenin was able to reduce the orange-peel appearance and increase microcirculation in a clinical study reported by Bertin et al.19 Single ingredients, also found in this formulation have documented anti-cellulite activity as well. This is the case for retinol, which by itself, improves skin thickness in patients with cellulite, as demonstrated clinically by Kligman et al,20 while Piérard-Franchimont et al21 reported effects on tensile properties of skin, in the context of cellulite. Acting to strengthen capillaries and limit edema when applied topically, escin, derived from horse chestnut, is another ingredient of the current gel that has found application in anti-cellulite formulations.22,23
+
The aim of the present study was to assess the clinical efficacy of a multi-active integral anti-cellulite gel, in comparison with a vehicle placebo gel, on a panel of human volunteers. Both products were evaluated and compared for their effect on tonicity, orange-peel aspect, stubborn cellulite, and their potential for reduction in circumference of areas affected by cellulite, over a period of 84 days.
Materials and methods
+
Products
+
The test product (from Immanence IDC Inc, Québec, QC, Canada) and the placebo (vehicle only) were supplied as gels of similar appearance and texture. Upon receipt by the testing laboratory, the samples were blindly assigned a code, before being stored at ambient humidity and temperature, in their original container. The active formulation contained several cosmetic actives selected on the basis of their potential to address all major mechanisms generally recognized as being involved in the development of cellulite (see Introduction and Table 1 for more details). The total concentration of cosmetic active ingredients in the formulation reached 25% (w/w). The placebo contained the exact formulation as the testing product, only without the active ingredients listed in Table 1, and consisted of a basic gel containing mainly water, jellifying agents, and preservatives.
Subjects
+
Forty-four healthy women, aged 25–55 years (mean age of 39.8 years), were recruited for this study. Twenty-two subjects (mean age of 39.1 years) were randomly assigned to the active product group, while the other 22 (mean age of 40.2 years) formed the placebo group. All subjects presented slight to moderate cellulite on their thighs, buttocks, and/or hips, at baseline. The subjects had a normal to slightly overweight BMI of between 20.0 and 28.0 kg m−2 and agreed to maintain their usual diet and level of physical activity throughout the study. People having taken, within 7 days of study start, medication, treatment, or natural products that could affect the outcome of the study, were excluded from the present protocol. Participants were asked to refrain from applying other anti-cellulite treatments, cosmetic products, or moisturizers to the studied areas for the duration of the study. Participants were neither allowed to receive additional massage treatment, nor to use any massage accessory during the whole length of the study. Participants were also instructed not to take medication or health supplements capable of affecting bodyweight for the length of the study.
Study design
+
The current study No 12F-0201 was a randomized, parallel-group, double-blind, placebo-controlled study, with one group assigned to the active gel and one group assigned to a placebo gel. Neither the participants nor the evaluators were aware of the nature (active or placebo) of the product being individually used. Subjects were instructed to apply the gel (active or placebo) on their hips, stomach, buttocks, and thighs, on a clean and dry skin, and to gently massage, with the palm only, until complete skin penetration. The procedure was repeated twice a day (morning and evening) for a total of 84 consecutive days (12 weeks). Clinical evaluation was performed in a laboratory room under controlled temperature (22°C±3°C) and relative humidity (30% ±5%), at day 0 (baseline), day 28 (week 4), day 56 (week 8), and day 84 (week 12). The weight of each volunteer was also recorded at each visit to determine their BMI and assess their compliance with protocol. The clinical data obtained at each time-point were compared with baseline for each group and also between groups in the search for statistically relevant differences. A self-assessment questionnaire was filled in on day 14 (week 2), day 28 (week 4), and day 84 (week 12) to document the subjects’ own subjective perception of product efficacy. The full detailed protocol is available from the sponsor of the study (Immanence IDC Inc).
Study location
+
The study took place in Montréal, Canada, from the end of February to the end of May, for a total of 84 consecutive days (12 weeks) following first application of the product. The study was conducted by an independent contract testing laboratory specialized in claim validation for cosmetic products, under the control of a dermatologist. The testing laboratory was responsible for the selection and randomization of all participants, as well as the gathering and statistical analysis of results.
Clinical assessment
+
Evaluation of skin tonicity
+
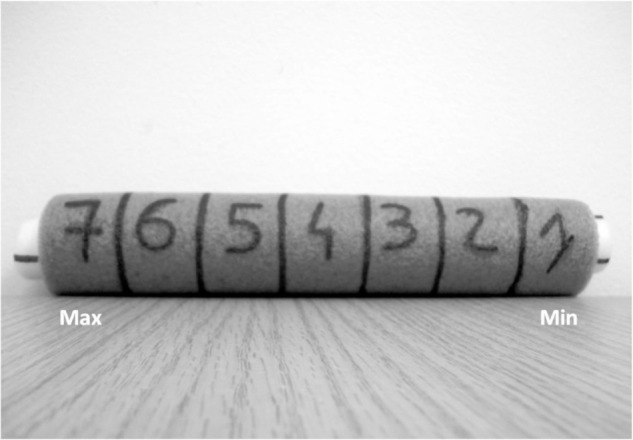
Skin tonicity was assessed using an analogical scale developed by the testing laboratory responsible for clinical evaluation of the product. For this purpose, a tubular device was designed and filled with layers of foam of increasing density in order to reproduce variations in skin tonicity, on a scale ranging from 1 “minimum firmness” to 7 “maximum firmness” (Figure 2). Grading of tonicity was performed by comparing the resistance of skin versus the resistance of this dedicated foam-like device, when applying a constant pressure with fingers. The repeatability and reproducibility of the procedure was validated by applying analysis of variance. In the present study, grading was performed by the same trained technician, on a precisely localized area of interest on hips, buttocks, and thighs.
+
Figure 2.
+
+
Device for grading skin tonicity. The tubular device is filled with layers of foam of increasing density in order to reproduce variations in skin tonicity, on a scale ranging from 1 “minimum firmness” to 7 “maximum firmness.” Grading is performed by comparing the resistance of skin versus the resistance of this dedicated foam-like device, when applying a constant pressure with fingers. The repeatability and reproducibility of the procedure has been validated by applying analysis of variance.
+
Abbreviations: Max, maximum; Min, minimum.
Evaluation of cellulite appearance
+
“Orange peel” aspect on relaxed skin and “stubborn cellulite” on pinched skin (thighs and hips) or on contracted buttocks were assessed using an analogical validated scale (from 0 “no intensity” to 8 “maximum intensity”) on hips, buttocks, and thighs (Figure 3). The scale used in the present study was an adaptation of a scale initially developed by Hexel et al.24 Orange peel and stubborn cellulite evaluation were performed by the same trained technician at each visit, in the same room (under controlled conditions of lighting, temperature, and humidity), and on the same body areas of interest for each subject, with the volunteer standing in a standardized upright position (ground references for feet repositioning).
+
Figure 3.
+
+
Visual grading scale for orange-peel appearance. The scale goes from 0 “no intensity” to 8 “maximum intensity.”
Each measurement site was localized precisely, with the help of a graduated rule and a laser beam to determine the site position with respect to the ground and ensure a correct vertical positioning. For reproducibility, the length of the laser beam was recorded at the first visit, and the same length was used at all subsequent visits. Additionally, a mapping of the skin’s surface features (eg, brown spots and scars) for each measurement site on each volunteer was recorded in order to precisely reposition during subsequent measurements.
Circumference measurements
+
Circumference measurements were obtained using a measuring tape, with the volunteers standing in a standardized upright position. Each measurement site was localized precisely, with the help of a graduated rule and a laser beam to determine the site position with respect to the ground and ensure a correct vertical positioning. For reproducibility, the length of the laser beam was recorded at the first visit, and the same length was used at all subsequent visits. Additionally, a mapping of the skin’s surface features (eg, brown spots and scars) for each measurement site on each volunteer was recorded in order to precisely reposition during subsequent measurements. The circumference of the following sites was measured: abdomen (2–3 cm below the navel), hips/buttocks, and both thighs (in the middle).
Qualitative survey
+
Treatment efficacy was also qualitatively assessed through a survey. The self-evaluation questionnaire was designed to gauge volunteers’ perception of the overall performance of products (active or placebo). All subjects were requested to fill in a questionnaire pertaining to skin firmness and smoothness on day 14 (week 2), as well as reduction of cellulite, attenuation of “orange skin” appearance, and improvement of skin texture on day 28 (week 4) and day 84 (week 12) of product application. Additionally, volunteers were asked to evaluate the perceived slimming effect after 84 days of twice-daily treatment. For a list of all evaluation criteria, please refer to Table 2.
+
Table 2.
+
Questionnaire and schedule for self-evaluation of product efficacy
+
+
+
Schedule
+
Criteria
+
+
+
+
Week 2 (day 14)
+
My skin seems smoother
+
+
My skin seems firmer
+
+
Week 4 (day 28)
+
The texture of my skin has improved (at touch)
+
+
My skin seems firmer
+
The “orange peel” appearance is attenuated
+
The signs of cellulite are visibly reduced
+
+
Week 12 (day 84)
+
The texture of my skin has improved (at touch)
+
+
My skin seems firmer
+
The “orange peel” appearance is attenuated
+
The signs of cellulite are visibly reduced
+
My skin seems more hydrated
+
My skin silhouette seems reshaped
+
My skin silhouette seems svelter
+
I feel like I have less water retention
+
My skin looks more radiant
+
+
+
Statistical analysis
+
Statistical analysis was carried out on all pertinent parameters. Results obtained at day 28, 56, and 84 for both treatments (test product and placebo) were compared with baseline results (day 0) using the Student’s t-test (paired two-sample t-test for means), allowing the evaluation of the effect of each treatment. Whenever appropriate, results were expressed as the mean of measurements obtained from all volunteers within each group. All relevant anti-cellulite results were noted and analyzed using a hypothesis test (two-sample t-test, assuming equal or unequal variance), allowing the comparison of the mean value of both groups at day 28 (week 4), day 56 (week 8), and day 84 (week 12), in order to determine whether there was any significant difference between the two treatments.
Ethics
+
The standard procedure and associated documents were reviewed and approved by the ethics committee of Evalulab Inc. prior to commencement of the clinical trial. The ethics committee was an independent organization whose members’ responsibility was to ensure the protection of the rights, security, and wellbeing of the volunteers participating in the study. Written informed consent was obtained from all participants prior to any trial procedure. This study was conducted in accordance with the ethical standards formulated in the 1964 Declaration of Helsinki and its later amendments.
Results
+
Participants
+
Of the 44 volunteers initially recruited, 40 completed the study. Two participants from each group (active and placebo) did not complete the study, the reason being unanticipated schedule incompatibilities. The remaining 40 volunteers completed the study without any adverse event and were included in the statistical analysis of the results by original assigned groups.
Efficacy results
+
Bodyweight evolution
+
The BMI of all volunteers did not vary significantly throughout the study. For the active product group, the average BMI was 24.8 kg m−2 at day 0 and 28, 24.6 kg m−2 at day 56, and 24.7 kg m−2 at day 84. For the placebo group, the average BMI was 24.5 kg m−2 at day 0, 24.7 kg m−2 at day 28, 24.6 kg m−2 at day 56, and 24.5 kg m−2 at day 84. Therefore, it is considered that all participants adhered to the protocol by maintaining their weight and lifestyle.
Evaluation of skin tonicity
+
After 84 days of twice-daily treatment the active gel significantly (P<0.05) improved skin tonicity, over baseline, on all studied areas (Figure 4). When compared with baseline, results reached average values of +9% at day 28, +39% at day 56, and +41% at day 84 on the buttocks. For hips, results gave average values of +10% at day 28, +17% at day 56, and +35% at day 84. For thighs, results were on average +9% at day 28, +17% at day 56, and +31% at day 84. Placebo treatment resulted in limited improvement of skin tonicity (Figure 4).
+
Figure 4.
+
+
Means of the evolution of skin tonicity at (A) day 28, (B) day 56, and (C) day 84 for both treated and placebo groups.
+
Notes: *Statistically significant versus baseline (P<0.05); §statistically significant versus placebo (P<0.05).
At day 84, statistical analysis (P<0.05) on all studied areas demonstrated that the active gel was better performing than placebo at increasing skin tonicity (Figure 4). Also, at the end of the study, a larger number of subjects presented improvement in skin tonicity when applying the active product, compared with placebo (95% versus 55% on thighs, 70% versus 40% on hips, and 70% versus 30% on buttocks) (Table 3).
+
Table 3.
+
Percentage of volunteers with improvement at the end of the study (day 84)
+
+
+
+
Zone
+
+
+
Thighs
+
+
+
Hips
+
+
+
Buttocks
+
+
+
Mean
+
+
+
+
+
Group
+
Active
+
Placebo
+
Active
+
Placebo
+
Active
+
Placebo
+
Active
+
Placebo
+
+
+
+
+
Tonicity
+
95%
+
55%
+
70%
+
40%
+
70%
+
30%
+
78%
+
42%
+
+
+
Orange peel
+
95%
+
40%
+
65%
+
10%
+
80%
+
20%
+
80%
+
23%
+
+
+
Stubborn cellulite
+
95%
+
40%
+
75%
+
20%
+
85%
+
35%
+
85%
+
32%
+
+
+
Mean
+
95%
+
45%
+
70%
+
23%
+
78%
+
28%
+
81%
+
32%
+
+
+
+
Evaluation of orange-peel appearance
+
After 84 days of product use, treatment with the active gel significantly (P<0.05) reduced the orange-peel appearance of the skin (no pinching), over baseline, on all studied areas (Figure 5). When compared with baseline, results obtained for buttocks reached average values of −9% at day 28, −16% at day 56, and −25% at day 84. For thighs, results were on average −5% at day 28, −11% at day 56, and −22% at day 84. For hips, results gave average values of −8% at day 56 and −22% at day 84. Placebo treatment resulted in limited improvement of orange-peel appearance (Figure 5).
+
Figure 5.
+
+
Means of the evolution of orange-peel appearance at (A) day 28, (B) day 56, and (C) day 84 for both treated and placebo groups.
+
Notes: *Statistically significant versus baseline (P<0.05); §statistically significant versus placebo (P<0.05).
At day 84, statistical analysis (P<0.05) on all studied areas demonstrated that treatment with the active gel was better performing at reducing the orange-peel appearance than placebo treatment (Figure 5). Also, at the end of the study, a larger number of subjects presented improvement in orange-peel appearance when applying the active gel, compared with placebo (95% versus 40% on thighs, 65% versus 10% on hips, and 80% versus 20% on buttocks) (Table 3).
Evaluation of stubborn cellulite appearance
+
After 84 days of product use, treatment with the active gel significantly (P<0.05) reduced stubborn cellulite (with pinching), over baseline, on all studied areas (Figure 6). When compared with baseline, results obtained for hips gave average values of −6% at day 28, −17% at day 56, and −24% at day 84. For thighs, the average values were −6% at day 28, −15% at day 56, and −22% at day 84. For buttocks, the average values were −9% at day 28, −15% at day 56, and −19% at day 84. Placebo treatment resulted in limited improvement of stubborn cellulite (Figure 6).
+
Figure 6.
+
+
Means of the evolution of stubborn cellulite (with pinching) at (A) day 28, (B) day 56, and (C) day 84 for both treated and placebo groups.
+
Notes: *Statistically significant versus baseline (P<0.05); §statistically significant versus placebo (P<0.05).
At day 84, statistical analysis (P<0.05) on all studied areas demonstrated that treatment with the active gel was better performing at reducing stubborn cellulite than placebo treatment (Figure 6). Also, at the end of the study, a larger number of subjects presented improvement in stubborn cellulite appearance when applying the active gel, compared with placebo (95% versus 40% on thighs, 75% versus 20% on hips, and 85% versus 35% on buttocks) (Table 3).
Circumference measurements
+
After 84 days of product use, treatment with the active gel significantly (P<0.05) reduced, over baseline, the circumference of all studied areas. When compared with baseline, results obtained for the abdomen gave average values of −0.4 cm at day 28, −0.9 cm at day 56, and −1.1 cm at day 84. For the right thigh, the average values were −0.3 cm at day 28, −0.6 cm at day 56, and −0.8 cm at day 84. For the left thigh, the average values were −0.1 cm at day 28, −0.4 cm at day 56, and −0.8 cm at day 84. For buttocks, the average values were −0.4 cm at day 28, −0.7 cm at day 56, and −0.8 cm at day 84 (Table 4). Placebo treatment resulted in limited improvement of circumference measurements (Table 4).
+
Table 4.
+
Means of the evolution (Dx–D0) of circumference measurements (in cm)
At day 84, statistical analysis (P<0.05) demonstrated that treatment with the active gel was better performing than placebo at reducing the circumference of the abdomen and thigh areas (Table 4). Also, at the end of the study, a larger number of subjects presented a reduction in circumference measurements on all studied areas when applying the active gel, compared with placebo (80% versus 35% on the abdomen, 45% versus 35% on the right thigh, and 70% versus 35% on the left thigh) (results not shown).
Qualitative survey
+
The overall scores for perceived performance of the test product (active gel or placebo) collected from the self-evaluation questionnaires completed by all volunteers are presented in Figure 7.
+
Figure 7.
+
+
Means of the evolution of self-perception of product efficacy at (A) day 14, (B) day 28, and (C) day 84 for both treated and placebo groups.
+
Notes: *Statistically significant versus baseline (P<0.05); §statistically significant versus placebo (P<0.05).
At day 14 and 28, statistical analysis of the data did not demonstrate any significant difference between the two groups in the perception of treatment efficacy.
+
At the end of the study (day 84), statistical analysis showed that the active gel performed significantly better than the placebo, on the following parameters (Figure 7).
+
+
Firmness: 85% versus 45% (P<0.05)
+
Orange peel appearance: 65% versus 25% (P<0.05)
+
Silhouette seems more svelte: 45% versus 15% (P<0.05)
+
+
At day 84, results reached near significance on the following parameters (Figure 7).
+
+
Silhouette seems reshaped: 50% versus 20% (P<0.1)
+
Less water retention: 40% versus 15% (P<0.1)
+
Signs of cellulite are visibly reduced: 55% versus 30% (P<0.1)
+
+
No statistical difference was observed for the other parameters.
Discussion
+
The present study was rigorously designed on a pharmaceutical model. This was a double-blind, parallel group, randomized, placebo-controlled study. The study establishes the efficacy of the test product (from Immanence IDC Inc) to improve the appearance of cellulite and reduce the circumference of the affected areas. At the end of the study period, statistical analysis on all pertinent parameters clearly demonstrated significant performance superiority for the active product over placebo. The test product was a gel integrating several cosmetic active ingredients (listed in Table 1) selected on the basis of their potential to address all major mechanisms generally recognized as being involved in the development of cellulite (Figure 1 and Table 1), according to published literature and/or patent documents. The formulation also covers all major skin aging mechanisms,14 since skin aging and cellulite may influence each other,12 as outlined in the Introduction.
+
By the end of the clinical trial (day 84), following twice-daily application of the test product, all studied parameters relating to cellulite, including skin tonicity, orange-peel appearance, and stubborn cellulite, were statistically improved over placebo (P<0.05) on all studied areas, ie, buttocks, thighs, and hips. Results obtained for skin tonicity reached average values of +41% for buttocks, +35% for hips, and +31% for thighs. Results obtained for orange-peel appearance (no pinching) reached average values of −25% for buttocks, −22% for hips, and −22% for thighs. Results obtained for stubborn cellulite (with pinching or on contracted buttocks) reached average values of −19% for buttocks, −24% for hips, and −22% for thighs. For the treated group, benefits were already seen on all parameters by day 28, improving constantly over time until the end of the study. The absence of a plateau effect suggests that the full potential for improvement had not been reached within 84 days (12 weeks) of twice-daily application of the test product, and that further amelioration might be seen with longer application periods.
+
At the end of the study (day 84), an average of 81% of the subjects applying the active gel presented improvement in their cellulite condition versus 32% for the placebo group (all descriptors and sites combined). The slight benefits obtained with the placebo gel are most likely related to a massaging effect upon application of the gel. Massaging is known to impact positively on cellulite appearance possibly by improving microcirculation and drainage in the affected area.25 In support of that, a combination of mechanical and manual lymphatic drainage has been reported to reduce body measurements in areas with cellulite.26 However, in the present study, the potential benefits from massaging are expected to be comparable for both groups since the placebo and treatment products contained the exact same gel base, had similar rheological characteristics, and were applied in the same manner.
+
The effect of the product on the appearance of the silhouette was assessed through circumference measurements of the abdomen, thighs, and hips/buttocks areas. By the end of the study (day 84), a significant reduction in circumference was observed over placebo (P<0.05) for the abdomen (mean of −1.1 cm) and for both thighs (mean of −0.8 cm). Again, limited benefits were obtained with the placebo gel; we believe this to reflect the contribution of massaging upon application. Importantly, all volunteers maintained a constant BMI throughout the study, attesting that the reduction in circumference and remodeling effects were not due to weight loss but most likely to better fluid drainage of the cellulite-affected areas and possibly also through a reduction in aging symptoms.
+
Treatment efficacy was also evaluated by the volunteers themselves. As could be expected, there was no difference in efficacy perception between the active product and the placebo group at day 14. Cellulite is a complex condition that cannot improve rapidly. However, slight differences between the two groups started emerging at day 28, and were neatly confirmed at day 84, with better performance for the active product over placebo. This progression in efficacy perception mirrors the progression documented through trained specialist evaluation. At the end of the study, statistically significant difference (Δ%) in terms of criteria appreciation between groups was seen for skin firmness, orange-peel appearance, and reshaped silhouette (Figure 7).
Conclusion
+
All results validate the efficacy of the present integral formulation to significantly reduce the signs of cellulite and reshape the silhouette, but do not provide information on the performance of individual ingredients within it. Cellulite is a complex phenomenon that requires a complex approach, and it is likely that no single ingredient is solely responsible for the benefits reported here. In support of this, synergistic action of anti-cellulite ingredients has been described in the literature previously.17–19,27,28 In fact, a multi-target/multi-component strategy is increasingly seen as the best approach to improve the appearance of cellulite.
+
Another limitation of the present study comes from the fact that it does not allow evaluating the contribution of anti-aging actives, found in the formulation, to the overall anti-cellulite effects. This could be the subject of future studies. The concept of fighting the appearance of cellulite by including both anti-aging and anti-cellulite actives in one integral formula is an interesting and promising approach that certainly deserves a closer look.
+
Yet another limitation of the study is linked to the fact that it was stopped before any plateau effect was reached. The maximum efficacy of the gel remains unknown, as well as its sustainability in time. More prolonged studies may be advisable in the future when assessing the effect of anti-cellulite products.
+
Nevertheless, the clear anti-cellulite beneficial effects of the blend of actives tested here support the use of a combination of ingredients exploiting different mechanisms of action and complementarily working to improve the condition.
Footnotes
+
+
Disclosure
+
ED owns Immanence IDC Inc (Québec, QC, Canada), the company that provided the test product and funded this research. JG is employed by the sponsor company, and DB is a paid consultant for the sponsor company. The other authors report no conflicts of interest in this work.
+
References
+
+
+1.Emanuele E, Bertona M, Geroldi D. A multilocus candidate approach identifies ACE and HIF1A as susceptibility genes for cellulite. J Eur Acad Dermatol Venereol. 2010;24(8):930–935. doi: 10.1111/j.1468-3083.2009.03556.x. [DOI] [PubMed] [Google Scholar]
+
+2.Rawlings AV. Cellulite and its treatment. Int J Cosmet Sci. 2006;28(3):175–190. doi: 10.1111/j.1467-2494.2006.00318.x. [DOI] [PubMed] [Google Scholar]
+
+3.Mirrashed F, Sharp JC, Krause V, Morgan J, Tomanek B. Pilot study of dermal and subcutaneous fat structures by MRI in individuals who differ in gender, BMI, and cellulite grading. Skin Res Technol. 2004;10(3):161–168. doi: 10.1111/j.1600-0846.2004.00072.x. [DOI] [PubMed] [Google Scholar]
+
+4.Kruglikov I. The pathophysiology of cellulite: can the puzzle eventually be solved? J Cosmet Dermatol Sci Appl. 2012;2(1):1–7. [Google Scholar]
+6.Terranova F, Berardesca E, Maibach H. Cellulite: nature and aetiopathogenesis. Int J Cosmet Sci. 2006;28(3):157–167. doi: 10.1111/j.1467-2494.2006.00316.x. [DOI] [PubMed] [Google Scholar]
+
+7.Khan MH, Victor F, Rao B, Sadick NS. Treatment of cellulite: Part I. Pathophysiology. J Am Acad Dermatol. 2010;62(3):361–370. doi: 10.1016/j.jaad.2009.10.042. [DOI] [PubMed] [Google Scholar]
+
+8.Hexsel D, Soirefmann M. Cosmeceuticals for Cellulite. Semin Cutan Med Surg. 2011;30(3):167–170. doi: 10.1016/j.sder.2011.06.005. [DOI] [PubMed] [Google Scholar]
+
+9.de la Casa Almeida M, Suarez Serrano C, Rebollo Roldán J, Jiménez Rejano JJ. Cellulite’s aetiology: a review. J Eur Acad Dermatol Venereol. 2013;27(3):273–278. doi: 10.1111/j.1468-3083.2012.04622.x. [DOI] [PubMed] [Google Scholar]
+
+10.Draelos ZD. The disease of cellulite. J Cosmet Dermatol. 2005;4(4):221–222. doi: 10.1111/j.1473-2165.2005.00194.x. [DOI] [PubMed] [Google Scholar]
+
+11.Pugliese PT. The pathogenesis of cellulite: a new concept. J Cosmet Dermatol. 2007;6(2):140–142. doi: 10.1111/j.1473-2165.2007.00312.x. [DOI] [PubMed] [Google Scholar]
+
+12.Ortonne JP, Zartarian M, Verschoore M, Queille-Roussel C, Duteil L. Cellulite and skin aging: is there any interaction? J Eur Acad Dermatol Venereol. 2008;22(7):827–834. doi: 10.1111/j.1468-3083.2007.02570.x. [DOI] [PubMed] [Google Scholar]
+
+13.Dupont E, Samson M, Galderisi A, inventors, Immanence Integral Dermo Correction Inc, assignee Skin care compositions and method of use thereof. 2011 Jun 30; United States patent US 20110158922. [Google Scholar]
+
+14.Dupont E, Gomez J, Léveillé C, Bilodeau D. From hydration to cell turnover: an integral approach to anti-aging. Cosmet Toiletries. 2010;125(3):50–60. [Google Scholar]
+
+15.Lupi O, Semenovitch IJ, Treu C, Bottino D, Bouskela E. Evaluation of the effects of caffeine in the microcirculation and edema on thighs and buttocks using the orthogonal polarization spectral imaging and clinical parameters. J Cosmet Dermatol. 2007;6(2):102–107. doi: 10.1111/j.1473-2165.2007.00304.x. [DOI] [PubMed] [Google Scholar]
+
+16.Kim C, Shim J, Han S, Chang I. The skin-permeation-enhancing effect of phosphatidylcholine: caffeine as a model active ingredient. J Cosmet Sci. 2002;53(6):363–374. [PubMed] [Google Scholar]
+
+17.Escudier B, Fanchon C, Labrousse E, Pellae M. Benefit of a topical slimming cream in conjunction with dietary advice. Int J Cosmet Sci. 2011;33(4):334–337. doi: 10.1111/j.1468-2494.2010.00630.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
+
+18.Roure R, Oddos T, Rossi A, Vial F, Bertin C. Evaluation of the efficacy of a topical cosmetic slimming product combining tetrahydroxypropyl ethylenediamine, caffeine, carnitine, forskolin and retinol, In vitro, ex vivo and in vivo studies. Int J Cosmet Sci. 2011;33(6):1–8. doi: 10.1111/j.1468-2494.2011.00665.x. [DOI] [PubMed] [Google Scholar]
+
+19.Bertin C, Zunino H, Pittet JC, et al. A double-blind evaluation of the activity of an anti-cellulite product containing retinol, caffeine, and ruscogenine by a combination of several non-invasive methods. J Cosmet Sci. 2001;52(4):199–210. [PubMed] [Google Scholar]
+
+20.Kligman AM, Pagnoni A, Stoudemayer T. Topical retinol improves cellulite. J Dermatolog Treat. 1999;10(2):119–125. [Google Scholar]
+
+21.Piérard-Franchimont C, Piérard GE, Henry F, Vroome V, Cauwenbergh G. A randomized, placebo-controlled trial of topical retinol in the treatment of cellulite. Am J Clin Dermatol. 2000;1(6):369–374. doi: 10.2165/00128071-200001060-00005. [DOI] [PubMed] [Google Scholar]
+23.Incandela L, Belcaro G, Nicolaides AN, Geroulakos G, Cesarone MR, De Sanctis MT. Microcirculation after standardized application of Essaven gel on normal skin – a placebo-controlled, randomized study. Angiology. 2001;52(Suppl 3):S5–S10. doi: 10.1177/0003319701052003S03. [DOI] [PubMed] [Google Scholar]
+25.Bayrakci Tunay V, Akbayrak T, Bakar Y, Kayihan H, Ergun N. Effects of mechanical massage, manual lymphatic drainage and connective tissue manipulation techniques on fat mass in women with cellulite. J Eur Acad Dermatol Venereol. 2010;24(2):138–142. doi: 10.1111/j.1468-3083.2009.03355.x. [DOI] [PubMed] [Google Scholar]
+
+26.de Godoy JM, de Godoy Mde F. Treatment of cellulite based on the hypothesis of a novel physiopathology. Clin Cosmet Investig Dermatol. 2011;4:55–59. doi: 10.2147/CCID.S20363. [DOI] [PMC free article] [PubMed] [Google Scholar]
+
+27.Al-Bader T, Byrne A, Gillbro J, et al. Effect of cosmetic ingredients as anticellulite agents: synergistic action of actives with in vitro and in vivo efficacy. J Cosmet Dermatol. 2012;11(1):17–26. doi: 10.1111/j.1473-2165.2011.00594.x. [DOI] [PubMed] [Google Scholar]
+
+28.Vogelgesang B, Bonnet I, Godard N, Sohm B, Perrier E. In vitro and in vivo efficacy of sulfo-carrabiose, a sugar-based cosmetic ingredient with anti-cellulite properties. Int J Cosmet Sci. 2011;33(2):120–125. doi: 10.1111/j.1468-2494.2010.00593.x. [DOI] [PubMed] [Google Scholar]
+32.Borel M, Calmon E, Bezivin C, Pletsch S, St Cyr JA. D-ribose enhances basal and mitochrondrial respiratory rates in human dermal fibroblasts. FASEB J. 2007;21(6):A835. [Google Scholar]
+
+33.Kawashima M, Mizuno A, Murata Y. Improvement of hyperpigmentation based on accelerated epidermal turnover: clinical effects of disodium adenosine monophosphate in patients with melasma. Jpn J Clin Dermatol. 2008;62:250–257. [Google Scholar]
+
+34.Furukawa F, Kanehara S, Harano F, et al. Effects of adenosine 5′-monophosphate on epidermal turnover. Arch Dermatol Res. 2008;300(9):485–493. doi: 10.1007/s00403-008-0882-x. [DOI] [PubMed] [Google Scholar]
+
+35.Ando H, Matsui MS, Ichihashi M. Quasi-drugs developed in Japan for the prevention or treatment of hyperpigmentary disorders. Int J Mol Sci. 2010;11:2566–2575. doi: 10.3390/ijms11062566. [DOI] [PMC free article] [PubMed] [Google Scholar]
+
+36.Burnstock G, Knight GE, Greig AV. Purinergic signaling in healthy and diseased skin. J Invest Dermatol. 2012;132(3 Pt 1):526–546. doi: 10.1038/jid.2011.344. [DOI] [PubMed] [Google Scholar]
+38.Thibodeau A. Protecting the skin from environmental stresses with an exopolysaccharide formulation. Cosmet Toiletries. 2005;120(12):81–89. [Google Scholar]
+
+39.Nusgens BV, Humbert P, Rougier A, et al. Topically applied vitamin C enhances the mRNA level of collagens I and III, their processing enzymes and tissue inhibitor of matrix metalloproteinase 1 in the human dermis. J Invest Dermatol. 2001;116(6):853–859. doi: 10.1046/j.0022-202x.2001.01362.x. [DOI] [PubMed] [Google Scholar]
+
+40.Kameyama K, Sakai C, Kondoh S, et al. Inhibitory effect of magnesium L-ascorbyl-2-phosphate (VC PMG) on melanogenesis in vitro and in vivo. J Am Acad Dermatol. 1996;34(1):29–33. doi: 10.1016/s0190-9622(96)90830-0. [DOI] [PubMed] [Google Scholar]
+
+41.Sauermann K, Jaspers S, Koop U, Wenck H. Topically applied vitamin C increases the density of dermal papillae in aged human skin. BMC Dermatol. 2004;4(1):13. doi: 10.1186/1471-5945-4-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
+
+42.Boyera N, Galey I, Bernard BA. Effect of vitamin C and its derivatives on collagen synthesis and cross-attachment linking by normal human fibroblasts. Int J Cosmet Sci. 1998;20(3):151–158. doi: 10.1046/j.1467-2494.1998.171747.x. [DOI] [PubMed] [Google Scholar]
+
+43.Xie Y, Chen X. Structures required of polyphenols for inhibiting advanced glycation end products formation. Curr Drug Metab. 2013;14(4):414–431. doi: 10.2174/1389200211314040005. [DOI] [PubMed] [Google Scholar]
+
+44.Caengprasath N, Ngamukote S, Mäkynen K, Adisakwattana S. The protective effects of pomelo extract (Citrus grandis L. Osbeck) against fructose-mediated protein oxidation and glycation. EXCLI J. 2013;12:491–502. [PMC free article] [PubMed] [Google Scholar]
+
+45.Leite Gde O, Leite LH, Sampaio Rde S, et al. (−)-α-Bisabolol attenuates visceral nociception and inflammation in mice. Fitoterapia. 2011;82(2):208–211. doi: 10.1016/j.fitote.2010.09.012. [DOI] [PubMed] [Google Scholar]
+
+46.Kamatou GPP, Viljoen AM. A review of the application and pharmacological properties of α-bisabolol and α-bisabolol-rich oils. J Am Oil Chem Soc. 2010;87:1–7. [Google Scholar]
+
+47.Mamalis A, Nguyen DH, Brody N, Jagdeo J. The active natural antioxidant properties of chamomile, milk thistle, and halophilic bacterial components in human skin in vitro. J Drugs Dermatol. 2013;12(7):780–784. [PubMed] [Google Scholar]
+
+48.Herrmann M, Meyer I, Joppe H, Vielhaber G. The Syngeristic Anti-irritant Effects of (−)-α-Bisabolol and Ginger. Cosmetics and Toiletries. 2007 Dec;122(7) [Google Scholar]
+
+49.Kim S, Lee J, Jung E, et al. Mechanisms of depigmentation by alpha-bisabolol. J Dermatol Sci. 2008;52(3):219–222. doi: 10.1016/j.jdermsci.2008.06.005. [DOI] [PubMed] [Google Scholar]
+
+50.Lee J, Jun H, Jung E, Ha J, Park D. Whitening effect of alpha-bisabolol in Asian women subjects. Int J Cosmet Sci. 2010;32(4):299–303. doi: 10.1111/j.1468-2494.2010.00560.x. [DOI] [PubMed] [Google Scholar]
+
+51.Herman A, Herman AP. Caffeine’s mechanisms of action and its cosmetic use. Skin Pharmacol Physiol. 2013;26(1):8–14. doi: 10.1159/000343174. [DOI] [PubMed] [Google Scholar]
+
+52.Jagdeo J, Brody N. Complementary antioxidant function of caffeine and green tea polyphenols in normal human skin fibroblasts. J Drugs Dermatol. 2011;10(7):753–761. [PubMed] [Google Scholar]
+
+53.Dayan N, Sivalenka R, Chase J. Skin moisturization by hydrogenated polyisobutene – quantitative and visual evaluation. J Cosmet Sci. 2009;60(1):15–24. [PubMed] [Google Scholar]
+
+54.Hexsel D, Zechmeister do Prado D, Rao J, Goldman MP. Topical management of cellulite. In: Goldman MP, Bacci PA, Leibaschoff G, Hexsel D, Angelinii F, editors. Cellulite: Pathophysiology and Treatment. New York: Taylor and Francis Group; 2006. pp. 159–170. [Google Scholar]
+
+55.Nayak BS, Ramdeen R, Adogwa A, Ramsubhag A, Marshall JR. Wound-healing potential of an ethanol extract of Carica papaya (Caricaceae) seeds. Int Wound J. 2012;9(6):650–655. doi: 10.1111/j.1742-481X.2011.00933.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
+
+56.Dayanand CD, Krishnamurthy N, Ashakiran S, Shashidhar KN. Carnitine: a novel health factor – an overview. Int J Pharm Biomed Res. 2011;2(2):79–89. [Google Scholar]
+
+57.Karsidag T, Asensio JA, Kabukcuoglu F, Tuzun S. Preliminary study comparing the effects of locally and systemically applied L-carnitine on the healing of full-thickness skin defects. Scand J Surg. 2010;99(3):147–152. doi: 10.1177/145749691009900309. [DOI] [PubMed] [Google Scholar]
+
+58.Wallimann T, Tokarska-Schlattner M, Schlattne U. The creatine kinase system and pleiotropic effects of creatine. Amino Acids. 2011;40(5):1271–1296. doi: 10.1007/s00726-011-0877-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
+
+59.Osamu T, Akinori H. The efficacy of L-carnitine on topical application for dry skin. The development of new active ingredient for dry skin as quasi-drug. Fragr J. 2005;33(8):82–85. [Google Scholar]
+
+60.Pillich RT, Scarsella G, Risuleo G. Reduction of apoptosis through the mitochondrial pathway by the administration of acetyl-L-carnitine to mouse fibroblasts in culture. Exp Cell Res. 2005;306(1):1–8. doi: 10.1016/j.yexcr.2005.01.019. [DOI] [PubMed] [Google Scholar]
+
+61.Parameshwaraiah S, Shivakumar HG. Evaluation of topical formulations of aqueous extract of Centella asiatica on open wounds in rats. Indian J Exp Biol. 1998;36(6):569–572. [PubMed] [Google Scholar]
+
+62.Haftek M, Mac-Mary S, Le Bitoux MA, et al. Clinical, biometric and structural evaluation of the long-term effects of a topical treatment with ascorbic acid and madecassoside in photoaged human skin. Exp Dermatol. 2008;17(11):946–952. doi: 10.1111/j.1600-0625.2008.00732.x. [DOI] [PubMed] [Google Scholar]
+
+63.Paolino D, Cosco D, Cilurzo F, et al. Improved in vitro and in vivo collagen biosynthesis by asiaticoside-loaded ultradeformable vesicles. J Control Release. 2012;162(1):143–151. doi: 10.1016/j.jconrel.2012.05.050. [DOI] [PubMed] [Google Scholar]
+
+64.Shukla A, Rasik AM, Dhawan BN. Asiaticoside-induced elevation of antioxidant levels in healing wounds. Phytother Res. 1999;13(1):50–54. doi: 10.1002/(SICI)1099-1573(199902)13:1<50::AID-PTR368>3.0.CO;2-V. [DOI] [PubMed] [Google Scholar]
+
+65.Garcia C, Stoltz C, inventors, SEPPIC, assignee Use of quinoa extract as cosmetic and pharmaceutic slimming agent and/or as an agent preventing the formation of new fats in the human body. 2010 Mar 11; United States patent US 20100061945 A1. [Google Scholar]
+67.Passeron T, Namiki T, Passeron HJ, Le Pape E, Hearing VJ. Forskolin protects keratinocytes from UVB-induced apoptosis and increases DNA repair independent of its effects on melanogenesis. J Invest Dermatol. 2009;129(1):162–166. doi: 10.1038/jid.2008.182. [DOI] [PMC free article] [PubMed] [Google Scholar]
+
+68.Peirano RI, Achterberg V, Düsing HJ, et al. Dermal penetration of creatine from a face-care formulation containing creatine, guarana and glycerol is linked to effective antiwrinkle and antisagging efficacy in male subjects. J Cosmet Dermatol. 2011;10(4):273–281. doi: 10.1111/j.1473-2165.2011.00579.x. [DOI] [PubMed] [Google Scholar]
+
+69.Lenz H, Schmidt M, Welge V, et al. The creatine kinase system in human skin: Protective effects of creatine against oxidative and UV damage in vitro and in vivo. J Invest Dermatol. 2005;124(2):443–452. doi: 10.1111/j.0022-202X.2004.23522.x. [DOI] [PubMed] [Google Scholar]
+
+70.Knott A, Koop U, Mielke H, et al. A novel treatment option for photoaged skin. J Cosmet Dermatol. 2008;7(1):15–22. doi: 10.1111/j.1473-2165.2008.00356.x. [DOI] [PubMed] [Google Scholar]
+
+71.Blatt T, Lenz H, Koop U, et al. Stimulation of skin’s energy metabolism provides multiple benefits for mature human skin. Biofactors. 2005;25(1–4):179–185. doi: 10.1002/biof.5520250121. [DOI] [PubMed] [Google Scholar]
+
+72.Kobayashi A, Shibazaki T. Manufacture and physiological activities of hydroxyproline. Fragr J. 2003;31(3):37–43. [Google Scholar]
+
+73.McNulty AK, Rhodes TJ, inventors, McNulty AK, Rhodes TJ., assignees Protease inhibitor compositions for prevention and treatment of skin conditions. 2005 Mar 3; United States patent US 20050048105 A1. [Google Scholar]
+
+74.Nagao S, Uehara K. Application to the cosmetics of amino acid derivatives. Fragr J. 2004;32(7):51–58. [Google Scholar]
+
+75.Hashizume E, Nakano T, Kamimura A, Morishita K. Topical effects of N-acetyl-L-hydroxyproline on ceramide synthesis and alleviation of pruritus. Clin Cosmet Investig Dermatol. 2013;6:43–49. doi: 10.2147/CCID.S39370. [DOI] [PMC free article] [PubMed] [Google Scholar]
+
+76.Lintner K, inventor, Sederma, Cosmetic or dermopharmaceutical compositions which are used to reduce bags and circles under the eyes. 2013 Aug 14; European patent EP 1474100 B1. [Google Scholar]
+
+77.Facino RM, Carini M, Stefani R, Aldini G, Saibene L. Anti-elastase and anti-hyaluronidase activities of saponins and sapogenins from Hedera helix, Aesculus hippocastanum, and Ruscus aculeatus: factors contributing to their efficacy in the treatment of venous insufficiency. Arch Pharm (Weinheim) 1995;328(10):720–724. doi: 10.1002/ardp.19953281006. [DOI] [PubMed] [Google Scholar]
+
+78.Luzzi R, Feragalli B, Belcaro G, et al. Aescin: microcirculatory activity. Effects of accessory components on clinical and microcirculatory efficacy. Panminerva Med. 2011;53(3 Suppl 1):51–55. [PubMed] [Google Scholar]
+
+79.Hexsel D, Orlandi C, Zechmeister do Prado D. Botanical extracts used in the treatment of cellulite. Dermatol Surg. 2005;31(7 Pt 2):866–872. doi: 10.1111/j.1524-4725.2005.31733. [DOI] [PubMed] [Google Scholar]
+
+80.Fujimura T, Tsukahara K, Moriwaki S, Hotta M, Kitahara T, Takema Y. A horse chestnut extract, which induces contraction forces in fibroblasts, is a potent anti-aging ingredient. J Cosmet Sci. 2006;57(5):369–376. [PubMed] [Google Scholar]
+
+81.Rosenthal RA, Fish B, Hill RP, et al. Salen Mn complexes mitigate radiation injury in normal tissues. Anticancer Agents Med Chem. 2011;11(4):359–372. doi: 10.2174/187152011795677490. [DOI] [PMC free article] [PubMed] [Google Scholar]
+
+82.Declercq L, Sente I, Hellemans L, Corstjens H, Maes D. Use of the synthetic superoxide dismutase/catalase mimetic EUK-134 to compensate for seasonal antioxidant deficiency by reducing pre-existing lipid peroxides at the human skin surface. Int J Cosmet Sci. 2004;26(5):255–263. doi: 10.1111/j.1467-2494.2004.00234.x. [DOI] [PubMed] [Google Scholar]
+
+83.Decraene D, Smaers K, Gan D, et al. A synthetic superoxide dismutase/catalase mimetic (EUK-134) inhibits membrane-damage-induced activation of mitogen-activated protein kinase pathways and reduces p53 accumulation in ultraviolet B-exposed primary human keratinocytes. J Invest Dermatol. 2004;122(2):484–491. doi: 10.1046/j.0022-202X.2004.22215.x. [DOI] [PubMed] [Google Scholar]
+
+84.Thibodeau A. The crucial role of metalloproteinase inhibitors and regenerating antioxidants in the age-related alterations of the skin. SOFW J. 2005;131(4):10–20. [Google Scholar]
+
+85.Paromov V, Kumari S, Brannon M, et al. Protective effect of liposome-encapsulated glutathione in a human epidermal model exposed to a mustard gas analog. J Toxicol. 2011;2011:109516. doi: 10.1155/2011/109516. [DOI] [PMC free article] [PubMed] [Google Scholar]
+
+86.Villarama CD, Maibach HI. Glutathione as a depigmenting agent: an overview. Int J Cosmet Sci. 2005;27(3):147–153. doi: 10.1111/j.1467-2494.2005.00235.x. [DOI] [PubMed] [Google Scholar]
+
+87.Fluhr JW, Darlenski R, Surber C. Glycerol and the skin: holistic approach to its origin and functions. Br J Dermatol. 2008;159(1):23–34. doi: 10.1111/j.1365-2133.2008.08643.x. [DOI] [PubMed] [Google Scholar]
+
+88.Draelos ZD. Active agents in common skin care products. Plast Reconstr Surg. 2010;125(2):719–724. doi: 10.1097/PRS.0b013e3181c83192. [DOI] [PubMed] [Google Scholar]
+
+89.Moon MH, Jeong JK, Lee YJ, et al. 18β-Glycyrrhetinic acid inhibits adipogenic differentiation and stimulates lipolysis. Biochem Biophys Res Commun. 2012;420(4):805–810. doi: 10.1016/j.bbrc.2012.03.078. [DOI] [PubMed] [Google Scholar]
+
+90.Armanini D, Nacamulli D, Francini-Pesenti F, Battagin G, Ragazzi E, Fiore C. Glycyrrhetinic acid, the active principle of licorice, can reduce the thickness of subcutaneous thigh fat through topical application. Steroids. 2005;70(8):538–542. doi: 10.1016/j.steroids.2005.01.007. [DOI] [PubMed] [Google Scholar]
+
+91.Afnan Q, Adil MD, Nissar-UlA, et al. Glycyrrhizic acid (GA), a triterpenoid saponins glycoside alleviates ultraviolet-B irradiation-induced photoaging in human dermal fibroblasts. Phytomedicine. 2012;19(7):658–664. doi: 10.1016/j.phymed.2012.03.007. [DOI] [PubMed] [Google Scholar]
+
+92.Asl MN, Hosseinzadeh H. Review of pharmacological effects of Glycyrrhiza sp and its bioactive compounds. Phytother Res. 2008;22(6):709–724. doi: 10.1002/ptr.2362. [DOI] [PMC free article] [PubMed] [Google Scholar]
+
+93.Graf J. Herbal anti-inflammatory agents for skin disease. Skin Therapy Lett. 2000;5(4):3–5. [PubMed] [Google Scholar]
+
+94.Saeedi M, Morteza-Semnani K, Ghoreishi MR. The treatment of atopic dermatitis with licorice gel. J Dermatolog Treat. 2003;14(3):153–157. doi: 10.1080/09546630310014369. [DOI] [PubMed] [Google Scholar]
+
+95.Cohen D, Heidary N. Treatment of irritant and allergic contact dermatitis. Dermatol Ther. 2004;17(4):334–340. doi: 10.1111/j.1396-0296.2004.04031.x. [DOI] [PubMed] [Google Scholar]
+
+96.Callender VD, St Surin-Lord S, Davis EC, Maclin M. Postinflammatory hyperpigmentation: etiologic and therapeutic considerations. Am J Clin Dermatol. 2011;12(2):87–99. doi: 10.2165/11536930-000000000-00000. [DOI] [PubMed] [Google Scholar]
+
+97.Goldman MP, Bacci PA, Leibaschoff G, Hexsel D, Angelinii F, editors. Cellulite: Pathophysiology and Treatment. New York: Taylor and Francis Group; 2006. [Google Scholar]
+
+98.Rai A. The antiinflammatory and antiarthritic properties of ethanol extract of Hedera helix. Indian J Pharm Sci. 2013;75(1):99–102. doi: 10.4103/0250-474X.113537. [DOI] [PMC free article] [PubMed] [Google Scholar]
+
+99.Gülçin I, Mshvildadze V, Gepdiremen A, Elias R. Antioxidant activity of saponins isolated from ivy: alpha hederin, hederasaponin-C, hederacolchiside-E and hederacolchiside-F. Planta Med. 2004;70(6):561–563. doi: 10.1055/s-2004-827158. [DOI] [PubMed] [Google Scholar]
+
+100.Koyuncu H, Berkarda B, Baykut F, et al. Preventive effect of hesperidin against inflammation in CD-1 mouse skin caused by tumor promoter. Anticancer Res. 1999;19(4B):3237–3241. [PubMed] [Google Scholar]
+
+101.Silva AR, Menezes PF, Martinello T, Novakovich GF, Praes CE, Feferman IH. Antioxidant kinetics of plant-derived substances and extracts. Int J Cosmet Sci. 2010;32(1):73–80. doi: 10.1111/j.1468-2494.2008.00483.x. [DOI] [PubMed] [Google Scholar]
+
+102.Hou M, Man M, Man W, et al. Topical hesperidin improves epidermal permeability barrier function and epidermal differentiation in normal murine skin. Exp Dermatol. 2012;21(5):337–340. doi: 10.1111/j.1600-0625.2012.01455.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
+
+103.Jin S, Zhou B, Luo D. Hesperidin promotes cyclobutane pyrimidine dimer repair in UVB-exposed mice epidermis. Ir J Med Sci. 2011;180(3):709–714. doi: 10.1007/s11845-010-0503-5. [DOI] [PubMed] [Google Scholar]
+
+104.Zhu W, Gao J. The use of botanical extracts as topical skin-lightening agents for the improvement of skin pigmentation disorders. J Investig Dermatol Symp Proc. 2008;13(1):20–24. doi: 10.1038/jidsymp.2008.8. [DOI] [PubMed] [Google Scholar]
+
+105.Li D, Mitsuhashi S, Ubukata M. Protective effects of hesperidin derivatives and their stereoisomers against advanced glycation end-products formation. Pharm Biol. 2012;50(12):1531–1535. doi: 10.3109/13880209.2012.694106. [DOI] [PubMed] [Google Scholar]
+
+106.Leite e Silva VR, Schulman MA, Ferelli C, et al. Hydrating effects of moisturizer active compounds incorporated into hydrogels: in vivo assessment and comparison between devices. J Cosmet Dermatol. 2009;8(1):32–39. doi: 10.1111/j.1473-2165.2009.00421.x. [DOI] [PubMed] [Google Scholar]
+
+107.Lu M, Duggan M, Menon G, Theophilus E, Dokka S, Wang H, inventors, Avon Prod Inc, assignee Topical cosmetic composition with skin rejuvenation benefits. 2008 Jul 2; European patent EP 1441686 B1. [Google Scholar]
+
+108.Agyare C, Dwobeng AS, Agyepong N, et al. Antimicrobial, antioxidant, and wound healing properties of Kigelia africana (Lam) Beneth and Strophanthus hispidus DC. Adv Pharmacol Sci. 2013;2013:692613. doi: 10.1155/2013/692613. [DOI] [PMC free article] [PubMed] [Google Scholar]
+
+109.Picerno P, Autore G, Marzocco S, Meloni M, Sanogo R, Aquino RP. Anti-inflammatory activity of verminoside from Kigelia africana and evaluation of cutaneous irritation in cell cultures and reconstituted human epidermis. J Nat Prod. 2005;68(11):1610–1614. doi: 10.1021/np058046z. [DOI] [PubMed] [Google Scholar]
+
+110.Oyedeji FO, Bankole-Ojo OS. Quantitative evaluation of the antipsoriatic activity of sausage tree (Kigelia africana) AJPAC. 2012;6(13):214–218. [Google Scholar]
+
+111.Morvan PY, L Pentecouteau L, Offredo H, Vallée R. Anti-ageing and slimming potential of a lotus maritimus extract via its effect on mitochondrial sirtuins on human skin cells; Proceedings of the 26th IFSCC Congress; September 20–23, 2010; Buenos-Aires, Argentina. [Google Scholar]
+
+112.Paufique J, inventor, SILAB, assignee Use of active ingredient comprising combination of active ingredient obtained from medicago sativa and active ingredient from Lupinus albus, to prepare cosmetic and/or dermopharmaceutical composition to fight against bags under the eyes. 2007 Oct 5; French patent FR 2921836-A1. [Google Scholar]
+
+113.Gaultier F, Foucault-Bertaud A, Lamy E, et al. Effects of a vegetable extract from Lupinus albus (LU105) on the production of matrix metalloproteinases (MMP1, MMP2, MMP9) and tissue inhibitor of metalloproteinases (TIMP1, TIMP2) by human gingival fibroblasts in culture. Clin Oral Investig. 2003;7(4):198–205. doi: 10.1007/s00784-003-0210-y. [DOI] [PubMed] [Google Scholar]
+
+114.Siger A, Czubinski J, Kachlicki P, Dwiecki K, Lampart-Szczapa E, Nogala-Kalucka M. Antioxidant activity and phenolic content in three Lupin species. J Food Comp Anal. 2012;25(2):190–197. [Google Scholar]
+
+115.Paufique J inventor, SILAB, assignee, editor. Active ingredient obtained from powdered Medicago sativa seeds. 2005 Aug 3; European patent EU 1559417A1. [Google Scholar]
+
+116.Paufique J, inventor, SILAB, assignee Method for obtaining a slimming cosmetic active agent, active ingredient obtained and composition including same. 2008 Jul 24; World patent WO2008087361 A2. [Google Scholar]
+
+117.Choulot JC, inventor, Caster, assignee Composition topique à visée amincissante. 2013 Jun 19; European patent EP 2604317 A1. [Google Scholar]
+
+118.Huang B, Zhu L, Liu S, et al. In vitro and in vivo evaluation of inhibition activity of lotus (Nelumbo nucifera Gaertn.) leaves against ultraviolet B-induced phototoxicity. J Photochem Photobiol B. 2013;121:1–5. doi: 10.1016/j.jphotobiol.2013.02.005. [DOI] [PubMed] [Google Scholar]
+
+119.Lupo MP. Peptides for facial skin aging. In: Shiffman MA, Mirrafati SJ, Lam SM, Cueteaux CG, editors. Simplified Facial Rejuvenation, Part III. Berlin: Springer Berlin Heidelberg; 2008. pp. 79–81. [Google Scholar]
+
+120.Maquart FX, Pickart L, Laurent M, Gillery P, Monboisse JC, Borel JP. Stimulation of collagen synthesis in fibroblast cultures by the tripeptide-copper complex glycyl-L-histidyl-Llysine-Cu2+ FEBS Lett. 1988;238(2):343–346. doi: 10.1016/0014-5793(88)80509-x. [DOI] [PubMed] [Google Scholar]
+
+121.Maquart FX, Bellon G, Pasco S, Monboisse JC. Matrikines in the regulation of extracellular matrix degradation. Biochimie. 2005;87(3–4):353–360. doi: 10.1016/j.biochi.2004.10.006. [DOI] [PubMed] [Google Scholar]
+
+122.Pickart L. The human tri-peptide GHK and tissue remodeling. J Biomater Sci Polym Ed. 2008;19(8):969–988. doi: 10.1163/156856208784909435. [DOI] [PubMed] [Google Scholar]
+
+123.Choi HR, Kang YA, Ryoo SJ, et al. Stem cell recovering effect of copper-free GHK in skin. J Pept Sci. 2012;18(11):685–690. doi: 10.1002/psc.2455. [DOI] [PubMed] [Google Scholar]
+
+124.Mas-Chamberlin C, Mondon P, Lamy F, Peschard O, Lintner K. In: Krisdaphong P, editor. Reduction of hair-loss: matrikines and plant molecules to the rescue; Proceedings of the 7th Scientific Conference of the Asian Society of Cosmetic Chemists (ASCS): Toward a New Horizon: Uniting Cosmetic Science with Oriental Wisdom; March 7-9, 2005; Bangkok, Thailand: Society of Cosmetic Chemists of Thailand; 2005. [Google Scholar]
+
+125.Lintner K, inventor, Sederma, assignee Utilisation cosmétique ou pharmaceutique de peptides pour la régulation des dysfonctionnements immunologiques et dans l’inflammation cutanée. 2000 Jul 27; World patent WO2000043417 A1. [Google Scholar]
+
+126.dal Farra C, Domloge N, Botto JM, inventors, ISP, assignee Dermatological and/or cosmetic composition containing polypeptides. 2008 Jul 17; United States patent US 20080171076 A1. [Google Scholar]
+
+127.dal Farra C, Berghi A, Oberto G, Domloge N. Significant in vivo slimming properties observed in new UCP-like peptide. J Am Acad Dermatol. 2007;56(2):AB88, P1015. [Google Scholar]
+
+128.Rios L, Delattre C, Chaisemartin L, Favre-Mercuret M, Berthon JY. A new generation of slimming products. SOFW J. 2012;138(11):1–11. [Google Scholar]
+
+129.Rios L, Delattre C, Patriarca P, Favre-Mercuret M, Berthon JY. A polyglucuronic acid to target the fiaf adipokine for slimming effects. Cosmet Toiletries. 2011;126(3):196–206. [Google Scholar]
+
+130.Darlenski R, Surber C, Fluhr JW. Topical retinoids in the management of photodamaged skin: from theory to evidence-based practical approach. Br J Dermatol. 2010;163(6):1157–1165. doi: 10.1111/j.1365-2133.2010.09936.x. [DOI] [PubMed] [Google Scholar]
+
+131.Kligman AM, Dogadkina D, Lavker RM. Effects of topical tretinoin on non-sun-exposed protected skin of the elderly. J Am Acad Dermatol. 1993;29(1):25–33. doi: 10.1016/0190-9622(93)70147-l. [DOI] [PubMed] [Google Scholar]
+
+132.Varani J, Warner RL, Gharaee-Kermani M, et al. Vitamin A antagonizes decreased cell growth and elevated collagen-degrading matrix metalloproteinases and stimulates collagen accumulation in naturally aged human skin. J Invest Dermatol. 2000;114(3):480–486. doi: 10.1046/j.1523-1747.2000.00902.x. [DOI] [PubMed] [Google Scholar]
+
+133.Kang S. The mechanism of action of topical retinoids. Cutis. 2005;75(Suppl 2):10–13. [PubMed] [Google Scholar]
+
+134.Wolf JE., Jr Potential anti-inflammatory effects of topical retinoids and retinoid analogues. Adv Ther. 2002;19(3):109–118. doi: 10.1007/BF02850266. [DOI] [PubMed] [Google Scholar]
+
+135.Bellemère G, Von Stetten O, Oddos T. Retinoic acid increases aquaporin 3 expression in normal human skin. J Invest Dermatol. 2008;128(3):542–548. doi: 10.1038/sj.jid.5701047. [DOI] [PubMed] [Google Scholar]
+138.Bellemère G, Stamatas GN, Bruère V, Bertin C, Issachar N, Oddos T. Antiaging action of retinol: from molecular to clinical. Skin Pharmacol Physiol. 2009;22(4):200–209. doi: 10.1159/000231525. [DOI] [PubMed] [Google Scholar]
+
+139.Sabancilar E, Aydin F, Bek Y, et al. Treatment of melasma with a depigmentation cream determined with colorimetry. J Cosmet Laser Ther. 2011;13(5):255–259. doi: 10.3109/14764172.2011.606463. [DOI] [PubMed] [Google Scholar]
+
+140.Merinville E, Byrne AJ, Visdal-Johnsen L, et al. Clinical evaluation of a dioic acid-based formulation on facial skin in an Indian population. Int J Cosmet Sci. 2012;34(6):575–581. doi: 10.1111/ics.12002. [DOI] [PubMed] [Google Scholar]
+
+141.Maswadeh HM, Semreen MH, Naddaf AR. Anti-inflammatory activity of Achillea and Ruscus topical gel on carrageenan-induced paw edema in rats. Acta Pol Pharm. 2006;63(4):277–280. [PubMed] [Google Scholar]
+
+142.Sharma S, Kaur IP. Development and evaluation of sesamol as an antiaging agent. Int J Dermatol. 2006;45(3):200–208. doi: 10.1111/j.1365-4632.2004.02537.x. [DOI] [PubMed] [Google Scholar]
+
+143.Hu Q, Xu J, Chen S, Yang F. Antioxidant activity of extracts of black sesame seed (Sesamum indicum L.) by supercritical carbon dioxide extraction. J Agric Food Chem. 2004;52(4):943–947. doi: 10.1021/jf034485x. [DOI] [PubMed] [Google Scholar]
+
+144.Suja KP, Jayalekshmy A, Arumughan C. Free radical scavenging behavior of antioxidant compounds of sesame (Sesamum indicum L.) in DPPH(*) system. J Agric Food Chem. 2004;52(4):912–915. doi: 10.1021/jf0303621. [DOI] [PubMed] [Google Scholar]
+
+145.Kiran K, Asad M. Wound healing activity of Sesamum indicum L seed and oil in rats. Indian J Exp Biol. 2008;46(11):777–782. [PubMed] [Google Scholar]
+
+146.Schlesinger TE, Powell CR. Efficacy and tolerability of low molecular weight hyaluronic acid sodium salt 0.2% cream in rosacea. J Drugs Dermatol. 2013;12(6):664–667. [PubMed] [Google Scholar]
+
+147.Pavicic T, Gauglitz GG, Lersch P, et al. Efficacy of cream-based novel formulations of hyaluronic acid of different molecular weights in anti-wrinkle treatment. J Drugs Dermatol. 2011;10(9):990–1000. [PubMed] [Google Scholar]
+
+148.Gariboldi S, Palazzo M, Zanobbio L, et al. Low molecular weight hyaluronic acid increases the self-defense of skin epithelium by induction of beta-defensin 2 via TLR2 and TLR4. J Immunol. 2008;181(3):2103–2110. doi: 10.4049/jimmunol.181.3.2103. [DOI] [PubMed] [Google Scholar]
+151.Chen WY, Abatangelo G. Functions of hyaluronan in wound repair. Wound Repair Regen. 1999;7(2):79–89. doi: 10.1046/j.1524-475x.1999.00079.x. [DOI] [PubMed] [Google Scholar]
+
+152.Merinville E, Byrne AJ, Rawlings AV, Muggleton AJ, Laloeuf AC. Three clinical studies showing the anti-aging benefits of sodium salicylate in human skin. J Cosmet Dermatol. 2010;(3):174–184. doi: 10.1111/j.1473-2165.2010.00506.x. [DOI] [PubMed] [Google Scholar]
+
+153.Weimar V. Polymorphonuclear invasion of wounded corneas; inhibition by topically applied sodium salicylate and soybean trypsin inhibitor. J Exp Med. 1957;105(2):141–152. doi: 10.1084/jem.105.2.141. [DOI] [PMC free article] [PubMed] [Google Scholar]
+
+154.Bair WB, 3rd, Hart N, Einspahr J, et al. Inhibitory effects of sodium salicylate and acetylsalicylic acid on UVB-induced mouse skin carcinogenesis. Cancer Epidemiol Biomarkers Prev. 2002;11(12):1645–1652. [PubMed] [Google Scholar]
+
+155.Lin AN, Nakatsui T. Salicylic acid revisited. Int J Dermatol. 1998;37(5):335–342. doi: 10.1046/j.1365-4362.1998.00452.x. [DOI] [PubMed] [Google Scholar]
+
+156.Huang ZR, Lin YK, Fang JY. Biological and pharmacological activities of squalene and related compounds: potential uses in cosmetic dermatology. Molecules. 2009;14(1):540–554. doi: 10.3390/molecules14010540. [DOI] [PMC free article] [PubMed] [Google Scholar]
+
+157.Wołosik K, Knaś M, Zalewska A, Niczyporuk M, Przystupa AW. The importance and perspective of plant-based squalene in cosmetology. J Cosmet Sci. 2013;(1):59–66. [PubMed] [Google Scholar]
+
+158.Kim SK, Bhatnagar I. Physical, chemical, and biological properties of wonder kelp-Laminaria. Adv Food Nutr Res. 2011;64:85–96. doi: 10.1016/B978-0-12-387669-0.00007-7. [DOI] [PubMed] [Google Scholar]
+
+159.Anton JG, Puche JC, Valles AG, Passerini E, inventors, Lipotec SA., assignee Composition for the prevention and treatment of cellulitis. 2007 Feb 8; United States patent US 20070031516 A1. [Google Scholar]
+
+160.Cals-Grierson MM. Modulation of activity of the adipocyte aquaglyceroporin channel by plant extracts. Int J Cosmet Sci. 2007;29(1):7–14. doi: 10.1111/j.1467-2494.2007.00351.x. [DOI] [PubMed] [Google Scholar]
+
+161.Mitani H, Ryu A, Suzuki T, Yamashita M, Arakane K, Koide C. Topical application of plant extracts containing xanthine derivatives can prevent UV-induced wrinkle formation in hairless mice. Photodermatol Photoimmunol Photomed. 2007;23(2–3):86–94. doi: 10.1111/j.1600-0781.2007.00283.x. [DOI] [PubMed] [Google Scholar]
+
+162.Ramiro E, Franch A, Castellote C, et al. Flavonoids from Theobroma cacao down-regulate inflammatory mediators. J Agric Food Chem. 2005;53(22):8506–8511. doi: 10.1021/jf0511042. [DOI] [PubMed] [Google Scholar]
+
+163.Sanbongi C, Osakabe N, Natsume M, Takizawa T, Gomi S, Osawa T. Antioxidative polyphenols isolated from Theobroma cacao. J Agric Food Chem. 1998;46(2):454–457. doi: 10.1021/jf970575o. [DOI] [PubMed] [Google Scholar]
+
+164.Gorouhi F, Maibach HI. Role of topical peptides in preventing or treating aged skin. Int J Cosmet Sci. 2009;31(5):327–345. doi: 10.1111/j.1468-2494.2009.00490.x. [DOI] [PubMed] [Google Scholar]
+
+165.Gruchlik A, Jurzak M, Chodurek E, Dzierzewicz Z. Effect of Gly-Gly-His, Gly-His-Lys and their copper complexes on TNF-alpha-dependent IL-6 secretion in normal human dermal fibroblasts. Acta Pol Pharm. 2012;69(6):1303–1306. [PubMed] [Google Scholar]
+
+166.Hussain M, Goldberg DJ. Topical manganese peptide in the treatment of photodamaged skin. J Cosmet Laser Ther. 2007;9(4):232–236. doi: 10.1080/14764170701704668. [DOI] [PubMed] [Google Scholar]
+
+167.Kang YA, Choi HR, Na JI, et al. Copper-GHK increases integrin expression and p63 positivity by keratinocytes. Arch Dermatol Res. 2009;301(4):301–306. doi: 10.1007/s00403-009-0942-x. [DOI] [PubMed] [Google Scholar]
+
+168.Zhang L, Falla TJ. Cosmeceuticals and peptides. Clin Dermatol. 2009;27(5):485–494. doi: 10.1016/j.clindermatol.2009.05.013. [DOI] [PubMed] [Google Scholar]
+
+169.Thiele JJ, Ekanayake-Mudiyanselage S. Vitamin E in human skin: organ-specific physiology and considerations for its use in dermatology. Mol Aspects Med. 2007;28(5–6):646–667. doi: 10.1016/j.mam.2007.06.001. [DOI] [PubMed] [Google Scholar]
+
+170.Kato E, Takahashi N. Improvement by sodium dl-α-tocopheryl-6-O-phosphate treatment of moisture-retaining ability in stratum corneum through increased ceramide levels. Bioorg Med Chem. 2012;20(12):3837–3842. doi: 10.1016/j.bmc.2012.04.029. [DOI] [PubMed] [Google Scholar]
+
+171.De Pascale MC, Bassi AM, Patrone V, Villacorta L, Azzi A, Zingg JM. Increased expression of transglutaminase-1 and PPARgamma after vitamin E treatment in human keratinocytes. Arch Biochem Biophys. 2006;447(2):97–106. doi: 10.1016/j.abb.2006.02.002. [DOI] [PubMed] [Google Scholar]
+
+172.Jain SK, Palmer M. The effect of oxygen radicals metabolites and vitamin E on glycosylation of proteins. Free Radic Biol Med. 1997;22(4):593–596. doi: 10.1016/s0891-5849(96)00377-2. [DOI] [PubMed] [Google Scholar]
+
+173.Muta-Takada K, Terada T, Yamanishi H, et al. Coenzyme Q10 protects against oxidative stress-induced cell death and enhances the synthesis of basement membrane components in dermal and epidermal cells. Biofactors. 2009;35(5):435–441. doi: 10.1002/biof.56. [DOI] [PubMed] [Google Scholar]
+
+174.Inui M, Ooe M, Fujii K, Matsunaka H, Yoshida M, Ichihashi M. Mechanisms of inhibitory effects of CoQ10 on UVB-induced wrinkle formation in vitro and in vivo. Biofactors. 2008;32(1–4):237–243. doi: 10.1002/biof.5520320128. [DOI] [PubMed] [Google Scholar]
+
+175.Hoppe U, Bergemann J, Diembeck W, et al. Coenzyme Q10, a cutaneous antioxidant and energizer. Biofactors. 1999;9(2–4):371–378. doi: 10.1002/biof.5520090238. [DOI] [PubMed] [Google Scholar]
+
+176.Prahl S, Kueper T, Biernoth T, et al. Aging skin is functionally anaerobic: importance of coenzyme Q10 for anti aging skin care. Biofactors. 2008;32(1–4):245–255. doi: 10.1002/biof.5520320129. [DOI] [PubMed] [Google Scholar]
+
+177.Grether-Beck S, Felsner I, Brenden H, et al. Urea uptake enhances barrier function and antimicrobial defense in humans by regulating epidermal gene expression. J Invest Dermatol. 2012;132(6):1561–1572. doi: 10.1038/jid.2012.42. [DOI] [PMC free article] [PubMed] [Google Scholar]
+
+178.Hagemann I, Proksch E. Topical treatment by urea reduces epidermal hyperproliferation and induces differentiation in psoriasis. Acta Derm Venereol. 1996;76(5):353–356. doi: 10.2340/0001555576353356. [DOI] [PubMed] [Google Scholar]
+
+179.Zhu K, Zhou H, Qian H. Antioxidant and free radical-scavenging activities of wheat germ protein hydrolysates (WGPH) prepared with alcalase. Process Biochemistry. 2006;41(6):1296–1302. [Google Scholar]
+
+180.Saraf S, Sahu S, Kaur CD, Saraf S. Comparative measurement of hydration effects of herbal moisturizers. Pharmacognosy Res. 2010;2(3):146–151. doi: 10.4103/0974-8490.65508. [DOI] [PMC free article] [PubMed] [Google Scholar]
+
\ No newline at end of file
diff --git a/docs/sources/pubmed-ncbi-nlm-nih-gov__15894038__d22fb9ab58.html b/docs/sources/pubmed-ncbi-nlm-nih-gov__15894038__d22fb9ab58.html
new file mode 100644
index 0000000..3a98eef
--- /dev/null
+++ b/docs/sources/pubmed-ncbi-nlm-nih-gov__15894038__d22fb9ab58.html
@@ -0,0 +1,280 @@
+
+
+
+
+
+
Glycyrrhetinic acid, the active principle of licorice, can reduce the thickness of subcutaneous thigh fat through topical application
+
+
+
+ Abstract
+
+
+
+
+
+ Cortisol is involved in the distribution and deposition of fat, and its action is regulated by the activity of 11beta-hydroxysteroid dehydrogenase. Glycyrrhetinic acid, the active principle of licorice root, blocks 11beta-hydroxysteroid dehydrogenase type 1, thus reducing the availability of cortisol at the level of adipocytes. We evaluated the effect of topical application of a cream containing glycyrrhetinic acid in the thickness of fat at the level of the thigh. Eighteen healthy women (age range 20-33 years) with normal BMI were randomly allocated to treatment, at the level of the dominant thigh, with a cream containing 2.5% glycyrrhetinic acid (n=9) or with a placebo cream containing the excipients alone (n=9). Before and after 1 month of treatment both the circumference and the thickness of the superficial fat layer of the thighs (by ultrasound analysis) were measured. The circumference and the thickness of the superficial fat layer were significantly reduced in comparison to the controlateral untreated thigh and to control subjects treated with the placebo cream. No changes were observed in blood pressure, plasma renin activity, plasma aldosterone or cortisol. The effect of glycyrrhetinic acid on the thickness of subcutaneous fat was likely related to a block of 11beta-hydroxysteroid dehydrogenase type 1 at the level of fat cells; therefore, glycyrrhetinic acid could be effectively used in the reduction of unwanted local fat accumulation.
+
Evaluation of the effects of caffeine in the microcirculation and edema on thighs and buttocks using the orthogonal polarization spectral imaging and clinical parameters
+
+
+
+ Abstract
+
+
+
+
+
+ Gynoid lipodystrophy, also known as cellulite, is a common multifactorial entity that affects millions of women around the world. There have been few scientific articles dealing with its physiology and treatment in the past few years, and vascular changes seem to play an important role in its pathophysiology. Skin microvascular alterations can be observed noninvasively with a new method called orthogonal polarization spectral imaging, which was used to evaluate the effectiveness of an anticellulite drug composed mainly of a 7% caffeine solution. Microcirculatory parameters evaluated were functional capillary density (FCD; number of flowing capillaries per unit area), diameter of the dermic papilla (DPD), and capillary diameter (CD). The clinical parameters analyzed were centimetrical measurements of thighs and hips and the influence of tobacco, alcohol, and physical activities on the efficacy of the treatment. After 1 month of treatment, statistical application of chi-squared and Z approximation tests showed, in treated patients, statistically significant reduction of thigh circumferences in more than 80% of the cases and reduction of hip circumference in 67.7%. FCD, DPD, and CD did not change significantly after treatment. Smoking as well as alcohol consumption and regular physical activity were not significantly related to the centimetrical reduction observed in treated thighs and hips.
+
Efficacy of Slimming Cream Containing 3.5% Water-Soluble Caffeine and Xanthenes for the Treatment of Cellulite: Clinical Study and Literature Review
+
+
+
+ Background:
+
+
+ Cellulite is a 'cottage cheese-like' cutaneous change caused by subcutaneous fat bulging into the dermis that usually leads to cosmetic problems. Slimming cream containing 3.5% water-soluble caffeine and xanthenes exhibits a lipolytic effect with penetration into the dermis.
+
+
+
+ Objective:
+
+
+ To evaluate the efficacy and safety of slimming cream for the treatment of cellulite.
+
+
+
+ Methods:
+
+
+ Fifteen subjects with cellulite applied slimming cream to the thighs and inner side of the upper arms twice daily for 6 weeks. Efficacy was assessed using a standard visual scale, changes in the circumferences of the thighs and upper arms, and patient satisfaction by a questionnaire at baseline, week 3, and week 6. Safety was assessed by inquiring about adverse events through questionnaires.
+
+
+
+ Results:
+
+
+ The standard visual scale score improved significantly by 0.49 points (19.8%) at week 6. Thigh and upper-arm circumferences decreased by 0.7 cm (1.7%) and 0.8 cm (2.3%), respectively, at week 6. Slight itching and transient flushing were commonly reported, but no serious adverse event occurred.
+
+
+
+ Conclusion:
+
+
+ The slimming cream tested appears to be effective for the treatment of cellulitis without serious adverse effects. However, additional large clinical trials are required to confirm the efficacy and safety of slimming cream for the treatment of cellulitis.
+
+
+
\ No newline at end of file
diff --git a/docs/sources/pubmed-ncbi-nlm-nih-gov__27060936__6e9bdde242.html b/docs/sources/pubmed-ncbi-nlm-nih-gov__27060936__6e9bdde242.html
new file mode 100644
index 0000000..d59b417
--- /dev/null
+++ b/docs/sources/pubmed-ncbi-nlm-nih-gov__27060936__6e9bdde242.html
@@ -0,0 +1,188 @@
+
+
+
+
+
+
A novel selective RF applicator for reducing thigh circumference: a clinical evaluation
+
+
+
+ Abstract
+
+
+
+
+
+ The demand for noninvasive body contouring procedures continues to drive the development of new technology to treat areas on the body that are more resistant to diet and exercise. This study assesses the safety and efficacy of a novel selective RF applicator as a noninvasive, contactless method for reducing thigh circumference using a radiofrequency electric field (Vanquish Flex Applicator, BTL Industries Inc., Boston, MA). Forty-two female subjects were enrolled to undergo a treatment of their bilateral inner and outer thighs (saddle bags) once weekly for 4 weeks. Thigh circumference was measured at the baseline and 2 weeks after the fourth treatment. The primary objective was the evaluation of clinical outcomes of 40 treated subjects. Safety of the device was assessed based on adverse events reports during the course of the study. Forty subjects completed the study. After four treatments, the therapy group showed a statistically significant (p < 0.001) reduction in thigh circumference of 2.43 cm compared with an untreated control group of 10 patients, where no change was seen (p = 0.297). No treatment associated pain or discomfort was reported by the subjects. There were also no reports of adverse events. This study demonstrates that the contactless RF Applicator is safe, painless and effective for the circumferential reduction of the thighs.
+